





Abstract
A 49-year-old woman presented to the hospital with a right inguinal swelling. On examination, we suspected hydrocele of the canal of Nuck (HCN) or an appendiceal or retroperitoneal tumor. Surgery for diagnosis and removal of the mass revealed that it was large and located in the preperitoneal cavity, extending into the inguinal ring; so, it was difficult to observe the entire outline of the mass solely using the laparoscopic approach. Therefore, we added the conventional approach with an inguinal incision. This combination of conventional and laparoscopic approaches helped in safe removal of the tumor. The HCN is an unusual developmental condition in women among whom it might cause an inguinal swelling infrequently. In a case with a large HCN, a combined approach using conventional and laparoscopic methods is suggested for better observation of the abdomen and successful resection without perforation of the mass than when using a single approach.
INTRODUCTION
The hydrocele of the canal of Nuck (HCN) is an unusual condition of female development that could manifest as an inguinal swelling [1]; however, precise diagnosis is difficult preoperatively [7]. Laparoscopic surgery had been performed for the diagnosis or treatment of this condition [2, 3]; however, large HCN is often difficult to excise using only the intra-abdominal approach of laparoscopic surgery owing to poor vision. Here, we successfully employed a combined surgical approach using conventional and laparoscopic methods for treatment of a large HCN.
CASE REPORT
A 49-year-old woman presented with painless swelling in her right inguinal region. She had a history of caesarian section and no history of infantile inguinal hernia. Physical examination revealed a soft egg-shaped mass extending from the right inguinal region to the labia majora. The mass was seen as a protrusion when the patient was in the standing position, while it disappeared when the patient was in the lying position. Ultrasound revealed a well-defined hypo-echoic elongated mass that extended from the superficial inguinal canal, with no solid component (Fig. 1). Computed tomography (CT) showed that 55 × 34 × 95 mm oval fluid collection located at the right inguinal region near the cecum and retroperitoneum in the abdominal cavity (Fig. 2). Total colonoscopy found no mucosal abnormalities from the cecum to the rectum; however, a mass of tissue pushed the cecal wall from outside (Fig. 3). This hinted toward a large HCN, appendiceal tumor or retroperitoneal tumor; we decided to attempt a combined approach of conventional and laparoscopic methods for diagnosis and treatment of the swelling. We used three ports (12, 10 and 5 mm; Fig. 4) for our laparoscopic approach. We placed a 12 mm laparoscopic trocar into the umbilicus for CO2 insufflation of the pneumoperitoneum. Endoscopic intraperitoneal observation revealed that the mass was distant from the cecum and outside the peritoneum (Fig. 5). The tumor was large and was not completely observed using only an intra-abdominal approach. Therefore, we used a combined approach, which was the conventional method with a skin incision in the inguinal region in addition to the intra-abdominal method with laparoscopic approach. The tumor could be resected without any damage by observing from both directions (Fig. 6). We adopted the Direct Kugel Patch (ONFLEX®, C.R. Bard, Inc., USA) for the vulnerability of the posterior wall of the inguinal canal. Histopathological examination revealed that the mass contained single-layered mesothelial cells and no tumor or endometriosis. Based on imaging, histopathology and operative findings, we diagnosed her with an HCN. The patient recovered and did not have any postoperative complications, and she was discharged from hospital on postoperative day 6. She had no recurrence of hernia or hydrocele until 16 months postoperatively.
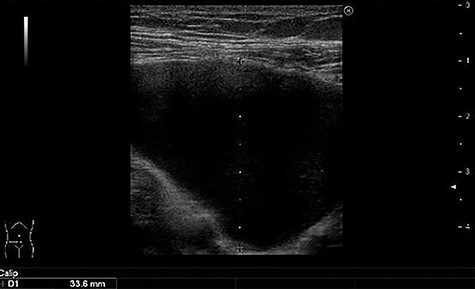
Well-defined, hypoechoic and elongated mass.
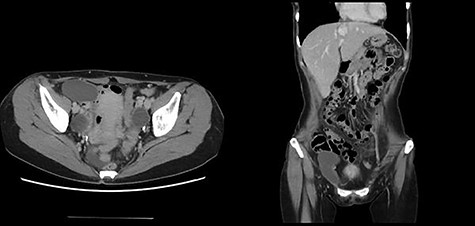
Oval fluid collection located in the right inguinal region.
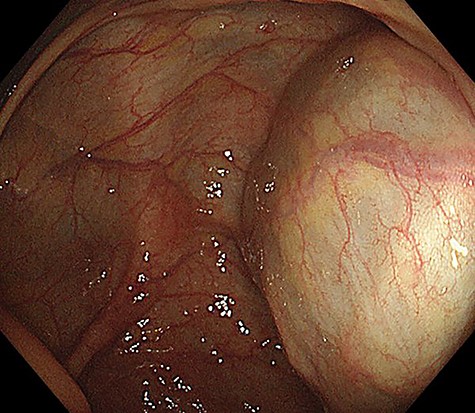
Colonoscopy image showing an unknown tissue mass that is pressed against the cecal wall from the outside.
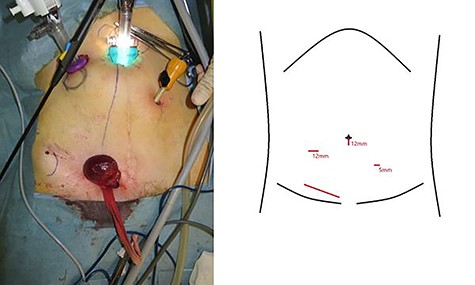
The three port sites and their dimensions.
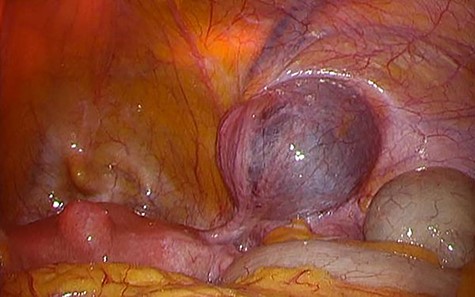
Laparoscopic finding.

Resected hydrocele.
DISCUSSION
The HCN is an unusual developmental condition in women in whom it may cause inguinal swelling infrequently.
Among women, extension of the parietal peritoneum follows the round ligament through the inguinal canal and internal ring. This evagination of the parietal peritoneum was named as the canal of Nuck and is the female equivalent to the processus vaginalis in men [5]. This evagination usually disappears after birth in both sexes but may result in indirect inguinal hernia if the peritoneal swelling remains. The hydrocele may present as a painless and elastic soft swelling in the inguinal region and labia majora [4]. Fluid hypersecretion or underabsorption may cause development of HCN. Such an imbalance result from factors, such as inflammation and trauma, but is mostly idiopathic [5]. The HCN does not have characteristic pathological findings. The canal of Nuck is divided into two layers: the outer wall comprising a fibrous tissue with variable thickness involving smooth muscle fibers, and the inner wall comprising single-layered mesothelial cells. Hypersecretion and malabsorption of fluid in the secretory membrane on the inner wall may form this hydrocele [6]. In our case, the mass contained single-layered mesothelial cells and no tumor or endometriosis. This finding is consistent with the diagnosis of HCN.
The combined approach with conventional and laparoscopic method is useful for diagnosis and treatment of large HCN.
It is very difficult to diagnose the HCN preoperatively. In cases where the HCN communicates with the peritoneal space, it often mimics an inguinal hernia in women because of its changeable mass [7]. There are many differential diagnoses for masses of the inguinal region besides HCN. Enlarged lymph nodes and soft tissue tumors (lipomas, leiomyoma and endometriosis of the round ligament) may cause inguinal or femoral hernias. In rare cases, vascular abnormalities, ganglion cysts, appendiceal tumor or retroperitoneal tumor may form the inguinal mass [4]. It would be difficult to diagnose the HCN solely based on physical findings [8]. In the present case, the tissue mass was huge, and we could not definitively diagnose it as HCN. Contrast-enhanced CT revealed a large oval fluid collection located in the inguinal region next to the cecum and retroperitoneum; thus, it was difficult to determine the exact origin of the cells from which the tumor could be derived. Because the mass could be potentially associated with an adverse abdominal condition (e.g. appendiceal or retroperitoneal tumor), it was necessary to identify the origin of the mass by observing the abdominal cavity.
Successful laparoscopic techniques in the diagnosis or treatment of the HCN have been reported [2, 3]. Our endoscopic observations were particularly useful in revealing that the hydrocele has no communication with the peritoneal cavity and was mainly located in the extraperitoneal space [2]. The tumor was large and was not seen completely using only the intra-abdominal approach. Therefore, we used a combined approach, including the conventional method with skin incision in the inguinal region and the intra-abdominal method with a laparoscopic approach. The tumor was resected without any damage by observing from both inside and outside.
To the best of our knowledge, this is the first report on the diagnosis and removal of a large HCN using a combined approach of conventional and laparoscopic methods. This technique may be useful for similar cases.
ACKNOWLEDGEMENTS
We would like to thank Editage (www.editage.jp) for English language editing.
Conflict of interest statement
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}