





ABSTRACT
Abdominoplasty is one of the most highly requested cosmetic procedures in the USA. Although it is famed for its cosmetic value, there are few reports that discuss its therapeutic potential. Furthermore, few abdominoplasties are completed in patients over the body mass index (BMI) of 30 due to fears of increased complications.
A 63-year-old male presented due to development of a large pannus following weight loss postgastric bypass. Unfortunately, because of this pannus, the patient began experiencing significant physical and emotional distress. The patient had difficult urinating, ambulating and could no longer engage in sexual activity. The patient underwent abdominoplasty for removal of the pannus. At the 5-month follow-up, patient exhibited resolution of his symptoms.
Abdominoplasty should not be limited to cosmetic procedures. It holds therapeutic value, and the BMI should not be listed as a firm contraindication to the procedure.
INTRODUCTION
Abdominoplasty is a procedure that is highly popular among individuals with recent significant weight loss. The procedure removes excess fat and skin. Although abdominoplasty is frequently performed on those with weight loss or postpregnancy changes, many plastic surgeons are hesitant to complete the procedure on obese patients, fearing the increased risk of possible complications [1, 2]. However, the relationship between obesity and certain diseases is more complex than we realize [3].
Many individuals who are obese suffer from significantly weakened abdominal musculature, resulting in functional disabilities and limitations [4]. The weakened musculature can contribute to the development of a significant pannus, drooping abdominal skin. Excessive drooping of the abdominal skin and abdominal wall laxity can result in severe reduction of quality of life. The resulting shift in the patient’s center of gravity can correspondingly cause back pain.
This case report examines a patient suffering from significant limitations in his daily activities due to his very large pannus. The patient was declined by multiple private and university-based practices in Las Vegas on the basis of his high body mass index (BMI) of 38.7 kg/m2. Because of his limited risk factors, aside from obesity, we elected to complete the abdominoplasty.
CASE PRESENTATION
A 63-year-old Caucasian male presented to the clinic for evaluation of a large abdominal pannus, which developed secondary to significant weight loss after having gastric sleeve surgery (Fig. 1). The patient reported difficulty urinating due to anatomical obstruction by pannus, relieved only by sitting down. He experienced significant difficulty ambulating due to discomfort from pannus sitting on his upper thighs and also rubbing against abdominal and pelvic skin. Furthermore, he could no longer engage in sexual activity with his partner. He reported having significant fatigue and back pain worsened by exertion and could no longer engage in exercise. Naturally, the patient experienced low self-esteem and anxiety due to distorted body image.
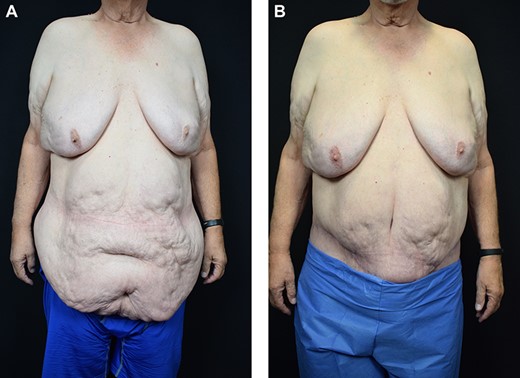
The patient anterior–posterior view before and after surgery.

The patient lateral view before and after surgery.
Significant past medical history included high blood pressure, diabetes and a gastric sleeve surgery in 2015. During physical exam, he was found to have a massive drooping belly and significant gynecomastia. The patient weighed 144.2 kg and his height was 1.93 m (BMI = 38.7 kg/m2). Patient’s preoperative labs, chest x-ray and echocardiogram were normal.
The patient’s abdomen was prepped from chest to midthigh. An incision was made along a prediagramed line, which followed the natural skin crease between the patient’s left and right anterior–superior iliac spines and extended posteriorly to correct lateral skin redundancy. Once the abdominal wall fascia was reached, dissection of the abdominal fat from the fascia proceeded superiorly and laterally to the level of the umbilicus. The umbilicus was carefully incised circumferentially.
Dissection of the abdominal flap proceeded to the xiphoid process in the midline and to the costal margin bilaterally. Next, the free and easily mobile skin flap was carefully drawn inferiorly. A surgical marking pen was used to diagram the amount of skin and fat, which would be excised. A transverse curvilinear incision was made, allowing for the redundant skin and adipose to be excised. The pannus was delivered to the back table and was found to weigh 9.48 kg (Fig. 3). A heavy nylon suture was used to reapproximate the medial edges of his rectus muscles. The position of the new umbilicus was marked, and an oval of skin was excised in the flap to allow the umbilicus to exit its new site without undue tension.
At 1-month follow-up, the patient reported satisfactory and improved ambulation and demonstrated a healed abdominal incision (Fig. 2). He was pleased and surprised by decreased fatigue on exertion. At 5-month follow-up patient reported ease of standing urination, exercise and sexual activity. The patient also reported a higher sense of self-esteem and positive self-image. Patient recovered well with no complications.
DISCUSSION
Abdominoplasty is one of the most widely used cosmetic procedures around the world. Strikingly, even with its higher rate of complications compared to other procedures, a retrospective study reported a 94.4% satisfaction rate among obese patients [5]. Yet, few reports exist of its therapeutic value. Although many surgeons express concern about increased risks associated with patients with a BMI > 30, retrospective chart review conducted upon 62 average BMI patients and 17 obese BMI patients of a plastic surgery practice in West Michigan exhibited no significant differences in perioperative complications from abdominoplasties [6]. Hence, patients should be examined for their other risk factors for complications—not just their obesity.
For this patient, his large drooping pannus resulted in severe limitations to his life and daily activities. It was the cause of his inability to have sexual relations, difficulty with urination and significant limitations in movement. These limitations precluded his ability to stay active and lose weight. By removing 9.48 kg of anterior pannus, the operation was able to decrease the obstructive pressures. The patient reported relief of his chronic back pain and improvement of his urinary obstruction. He also reported resolution of his chronic fatigue, which may have been linked to the decreased abdominal pressure and poor back stability from the heavy pannus.

The removed tissue specimen after surgery (9.480 kg).
The abdominoplasty functioned as a way of removing the pannus and increasing the strength of his relatively weak abdominal musculature. A study completed in Turkey suggested that the surgery allowed for change in the center of gravity and increased abdominal pressure [4]. These factors reportedly create a more stable vertebral column, which can more effectively support the body’s weight.
In conclusion, as healthcare providers, it is imperative to evaluate patients on the basis of more than just their BMI. Completion of abdominoplasty in an obese patient, especially in patients with weakened musculature, can prove more therapeutic and beneficial than simple recommendations of weight loss and exercise. In the case of the aforementioned patient, abdominoplasty improved the quality of life and resolved his chronic pain, difficulty ambulating and urinary obstruction.
FUNDING
None declared.
CONFLICT OF INTEREST STATEMENT
None declared.
ETHICAL APPROVAL
Yes.
CONSENT
Yes.

{kind=link}
{kind=link}
{kind=link}