





Abstract
Congenital malformations of the thumb greatly affect the performance of the hand and the upper limb. The conditions associated with atrophic thumb represent a wide spectrum of abnormalities, ranging from a complete absence to a mere small size of the thumb. A 5-year-old Caucasian female presented with congenital clasped thumb deformity with hypoplastic thumb and with an absence of extrinsic extensors extensor pollicis longus and brevis and with stable carpometacarpal joint. We managed this case by transferring the extensor indicis proprius tendon and flexor digitorum superficialis of digitus medicinalis (the ring finger)—which is not common—to compensate for the absence of extension and abduction tendons of the thumb. After 17 years, the result was satisfactory for the patient and her family. She was able to use her hand for writing and doing normal daily work without feeling any disability.
INTRODUCTION
The congenital clasped thumb is an unusual condition in which the thumb is positioned in adduction and extreme flexion at the metacarpophalangeal joint and interphalangeal joints.
There is no single cause, the deformity results from an imbalance between the flexors and extensors of the thumb.
If no active extension at the metacarpophalangeal joint is shown after prolonged observation and particularly by the age of 3 months, the diagnosis of congenital clasped thumb is established [1].
Initial treatment is splinting, which is objectively effective in children younger than 1 year of age.

First examination and evaluation.
Surgery is indicated for children who have failed splinting or who present at an older age and have a functional impairment [2]. This may be an isolated deformity or associated with other deformities and syndromes [1].
We report a rare case of congenital clasped thumb in a 5-year-old Syrian girl with the absence of extensor pollicis brevis and longus (EPB and EPL) and with stable carpometacarpal (CMC).
CASE REPORT
A 5-year-old Caucasian female presented to the outpatient clinic with her parents in 2001 complaining of being unable to use a pen with her right hand.
At first examination, the thumb was seen at adduction and flexion position, it cannot be extended, and after passive extension, it returns to original adduction and flexion position (Fig. 1).
There was a contracture and absence at the first web and the thumb was smaller than the opposite left one.
There was no extension in the interphalangeal joint due to the absence of EPL, also in the metacarpophalangeal joint due to the absence of EPB, whereas the CMC joint was stable.

X-ray imaging of the right hand showed small-sized bones of the right thumb including first metacarpal and phalanges, it also showed the good alignment of the CMC and MCP joints.

During the surgery.
The following movements: flexion, adduction and opposition were within normal.
Neither stiffness nor instability in interphalangeal (IP) or metacarpophalangeal (MCP) joints was observed (Fig. 2).
The deformity was isolated as no bones were missing in her body and she was not suffering from any syndromes. Also, no similar cases were reported in her family history.
We ensured the diagnosis of congenital clasped thumb deformity with hypoplastic thumb. We did not face any difficulty with the differential diagnosis between this situation and neonatal trigger thumb because of the late presence of the patient at the age of 5 years. The late presence and the absence of EPL and EPB made the conservative treatment with splinting no more successful and the reconstructive surgery the only proper way to achieve good results.
The surgery was performed in one stage, it took 90 min under general anesthesia, a tourniquet was applied on the upper right arm and the first web was obtained by performing an expansion surgery with simple z-plasty. Then, a drill-hole was made in the base of the proximal phalanx of the thumb, where the extensor indicis proprius (EIP) tendon was passed through and sutured to itself, while the end of the flexor digitorum superficialis (FDS) of the ring finger was sewed to the end of the distal phalanx and fixed with a button, and the thumb was placed at full abduction and extension position and fixed with a K-wire (Kirschner wire) inserted from distal to proximal (Fig. 3).
A supporting splint of the forearm and thumb was applied and then replaced with below elbow cast after removing the stitches two weeks after the surgery (Fig. 4).
Six weeks later, the cast and the K-wire were removed. Six months later, she was able to hold a pen and write with good flexion and extension of the thumb (Fig. 5). The patient was examined in 2018 (Fig. 6).

Two weeks after the surgery, after removing the stitches.
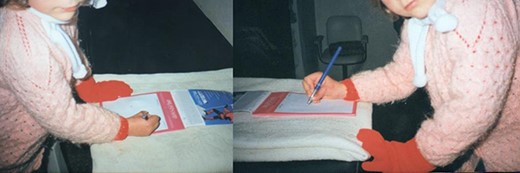
Six months after the surgery, she was able to hold a pen and write with good flexion and extension of the thumb.

Seventeen years after the surgery (in 2018). The smallness of the thumb was observed, the extension and abduction of the thumb had a good range of motion with a sufficient pinch grip and were sufficient for her to become a university student.
DISCUSSION
Blauth classification [3] separates thumb deficiencies into five types. Type I is minor generalized hypoplasia. In type II, there are an absence of intrinsic thenar muscles, narrowing at the first web space and insufficiency at the ulnar collateral ligament. Type III has similar findings as type II in addition to extrinsic muscle and tendon abnormalities and skeletal deficiency. Type III is subdivided into types IIIA with stable CMC joint and IIIB with unstable CMC joint. Type IV represents a profound deficiency known as a pouce flottant. Type V is complete absence of the thumb.
Our case is considered type IIIA because of the absence of EPL and EPB, and the stability of CMC joint.
Tsuyuguchi et al [4] separated this syndrome into three groups. Type I is the flexible type in which thumb can be passively extended with no other abnormality. In type II, thumb cannot be passively abducted or extended, and skin contracture, and there is comorbid collateral ligament or thenar muscle abnormalities. Type III occurs together with arthrogryposis.
Our case is considered type I as the passive extension and abduction could be carried out.
Sancar Serbest et al [5] reported that good results were achieved with EIP only transfer and z-plasty reconstruction to the first web space.
But in our method, we transferred ‘two’ tendons (EIP and FDS of the ring finger) to compensate for the absence of EPL and EPB, which is not common.
CONCLUSION
Congenital clasped thumb syndrome should be kept in mind in cases with flexion and adduction deformity; in cases of tendon hypoplasia or absence who presented late and have contracture at the first web space, EIP and FDS of the ring finger tendons transfer and z-plasty of contracture in first web interval is a successful method in order to achieve very good functional result.
ACKNOWLEDGEMENTS
We are grateful to Dr Ziad Aljarad and Dr Marwa Aloulou for her help in reviewing the manuscript and also to Dr Usama Dib for his help in the manuscript editing.
Conflict of interest statement
None declared.
FUNDING
No funding was required.
ETHICAL APPROVAL
Not required for this case report.
CONSENT
The patient and her father declared that they have no problem in publishing the case.
GUARANTOR
A.Z. is the guarantor of this work.
References
Author notes
Co-author: Abdulmouain Zrek, head of Orthopaedic Surgery Department, Al-Razi Hospital, Aleppo, Syria.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}