





Abstract
The causes of dysphonia or hoarseness are numerous and can be classified as functional or organic. The report will highlight the clinical presentation, histopathological features and management plan of laryngeal epidermal inclusion cysts (EICs). Laryngeal EICs are rare. The epidermal and dermoid cysts represent only 0.01% of oral cavity cysts. Their clinical presentation varies from a completely asymptomatic presentation to dysphonia for years. This current report represents a case of a 34-year-old female who presented with 2-year history of dysphonia, which was caused by a unilateral laryngeal EIC.
INTRODUCTION
Epidermal inclusion cysts (EIC) are benign cysts containing keratin fibers and are lined by almost an identical histology to the skin epidermis [1], Also, it is analogous to cholesteatoma in the histologic structure [2]. Generally, laryngeal cysts comprise only 5% of all benign laryngeal lesions [3]. EIC are rarely encountered in the larynx as only 0.01% of oral cavity cysts are epidermoid and dermoid cysts [1]. The clinical presentation varies as some patients are asymptomatic unlike others complain of chronic dysphonia or hoarseness. However, in a review article Polyps and cysts represented only 10.7–31% of the causes of dysphonia [4]. We report the case of a right vocal fold EIC in a female patient. The clinical and histopathologic characteristics of the patient’s presentation are described and discussed.
CASE REPORT
A 34-year-old female patient, who is not known to have any medical or surgical illnesses, presented to the otolaryngology clinic complaining of hoarseness, chronic cough and frequent throat clearing. There was no history of heartburn. On physical examination: The vital signs were within normal limits. Cervical lymph nodes were not palpable.
The patient is a housewife who does not smoke nor drink alcohol.
Laryngeal videostroboscopy was done and it showed bilateral intrachordal cysts with bilateral mild edema, erythema and hypertrophy of both arytenoids.
The mobility of both right and left vocal cords was normal with no restriction. The right vocal cord cyst was larger in size.
The patient underwent bilateral vocal cord cyst excision under the assistance of a micro laryngoscope, the procedure was performed under general anesthesia, prepping and draping were done in sterile fashion.
Anterior commissure laryngoscope was used, and suspension was done. Starting by the right-side cyst, an incision was made lateral to the cyst using a sickle knife, followed by dissection around the cyst using a micro dissector, and then resection was done using a micro-scissor. The left side lesion was excised using the exact technique but the lesion was excised in fragments.
The patient was stable postoperatively and the postoperative plan included voice rest for 10 days, continuation of proton pump inhibitor uses and voice therapy.
Upon follow-up, which was 20 days and 3 months postoperatively, the patient was asymptomatic, and the vocal cords were bilaterally mobile with no residual cysts.
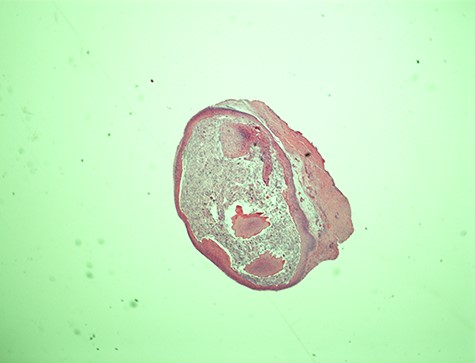
Epidermal cyst—20× magnification. Low power microscopic view of the vocal cord epidermal inclusion cyst. Hematoxylin and eosin (H&E) stain X.
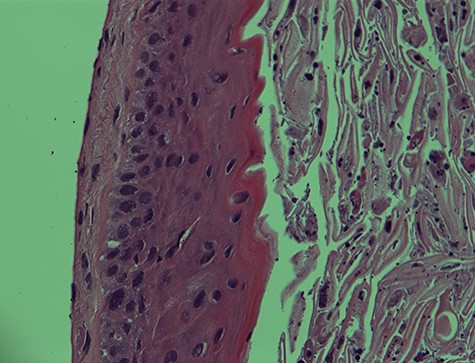
I. Epidermal cyst—400× magnification. EIC of the vocal cord. Note the undulating lining squamous epithelium with numerous keratinous and cellular debris in the lumen. H&E stain X400.
HISTOPATHOLOGICAL FEATURES
The histopathological features of the right vocal cord cyst were consistent with an EIC of the larynx, whereas the left vocal cord cyst showed minute fragment of benign squamous epithelium and skeletal muscle (Figs 1 and 2).
Both right and left vocal cord cysts were negative for dysplasia and malignancy.
P16 immunohistochemical stain was performed, and it was negative.
DISCUSSION
The causes of Dysphonia or hoarseness are numerous and can be classified as functional or organic. The organic causes include: “structural (e.g., vocal fold nodules, polyps, cysts, laryngeal papillomatosis, premalignant and malignant pathology) or neurological abnormality of larynx” [5].
The most commonly detected pathologies in Van Houtte et al. [5] study population were 30% functional voice disorders, 15% vocal fold nodules, pharyngolaryngeal reflux with laryngitis in 9 and 8% polyps and cysts of the larynx. Functional voice disorders are the main cause of dysphonia in all age groups, starting from the age of 15 years, to the age of > 64 years.
Laryngopharyngeal reflux (LPR) is being proposed primarily in the differential diagnosis list especially in patients who have associated symptoms of: Throat clearing, excess mucus, cough, globus and heartburn. However, it was proposed by Rafii et al. [6] that in two-thirds of the initially diagnosed patients (LPR) have an underlying discrete laryngeal pathology such as mucosal benign lesions, vocal cord paralysis or neoplastic lesions [6].
The pathophysiology of the development of laryngeal cysts involves mechanical traumas leading to the development of a wound, which undergoes remodeling which changes the nature at the superficial level of lamina propria and the development of the cyst Johns et al [7].
Approaching dysphonia requires proper history, examination and investigations.
Risk factors and red flags of laryngeal cancers have to be ruled out, such as consumption of alcohol and cigarettes smoking [8]. As laryngeal cancer is the second most common respiratory cancer and the most prevalent type of laryngeal cancer is glottic.
The early symptoms of vocal fold cysts are hoarseness, reduced voice volume and vocal fatigue.
Finally, microsurgical cyst excision and voice therapy are the pillars of management of laryngeal EIC; this management plan is supported by the concept that there is functional aspect contributing to the development of these cysts as was proposed by a case series of Milutinović Z [9], in which the cysts were found on the most active vocal fold at its free edge at the anteromiddle of the vocal fold, and patients were characterized by having hyperkinetic voice production [9]. The location of the cyst was also described in Bouchayer et al. [10] case series and Johns et al. [7] as being most commonly at the middle portion of vocal fold by laryngeal videostroboscopy.
In conclusion, EIC is a rare benign glottic lesion. It usually results from a trauma to the vocal cords. Patients present clinically with chronic dysphonia; Laryngeal videostroboscope is able to identify the cysts. The management plan includes voice rest, voice therapy and microlaryngoscopic excision in persisting cases.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}