





Abstract
Behçet’s disease (BD) is a multisystemic, immune-mediated occlusive vasculitis of unknown etiology with a chronic, relapsing remitting course. Ocular involvement is characterized by recurrent nongranulomatous uveitis with necrotizing obliterative vasculitis affecting both the anterior and posterior segments of the eye and often leads to blindness.
We describe successful surgical management of a rare case of combined rhegmatogenous retinal detachment (RRD) and tractional retinal detachment (TRD) in a patient with Behçet’s disease.
A 28-year-old Hispanic women with known Behcet’s disease presented with loss of vision of both eyes. She was found to have extensive bilateral necrotizing vasculitis with severe ischemia. Despite aggressive antivascular endothelial growth factor (VEGF) therapy and pan retinal photocoagulation, patient progressed to total blindness from development of combined rhegmatogenous and tractional funnel retinal detachment. Small gauge pars plana vitrectomy (PPV) with silicone oil tamponade was performed for retinal detachment repair (without scleral buckle).
Combined RRD and TRD was successfully treated with standard PPV with silicone oil placement without use of scleral buckle. Visual acuity 1 year postoperatively improved from ability to perceive light to 20/400.
Combined forms of retinal detachment, a rare development in Behçet’s disease may be effectively treated with PPV (without scleral buckling) with favorable visual and anatomic outcomes.
INTRODUCTION
Adamantiades-Behçet’s disease (BD) is a multisystemic, immune-mediated occlusive vasculitis of unknown etiology with often a chronic, relapsing remitting course [1]. Due to its systemic nature, clinical presentation is variable and includes cutaneous, joint, and less commonly, gastrointestinal, neurological, and cardiovascular manifestations. The International Study Group for Behçet’s disease diagnostic criteria mandates the presence of oral ulceration plus any two of the following: genital ulceration, typical defined eye lesions, skin lesions or a positive pathology test [2]. Most commonly, patients present with oral aphthous ulcers, genital ulcers and ocular disease [3, 4]. Despite its worldwide distribution, most cases are reported in the Middle East, Mediterranean region and the Far East, particularly Japan [3, 5]. Though the exact pathogenesis remains unclear, a relationship between BD and complex genetic factors perpetuating inflammation, such as presence of the HLA B-51 haplotype, have been reported [1].
Ocular involvement carries one of the most serious implications of BD due to poor visual prognosis despite immunosuppressive therapy occurring in 43–80% of patients [1, 3]. It is characterized by recurrent nongranulomatous uveitis with necrotizing obliterative vasculitis affecting both the anterior and posterior segments of the eye [3]. Though the disease process affects the entire globe, vitreoretinal complications in patients with BD are often the most severely sight-threatening [3]. Posterior segment sequelae of BD requiring surgical management include persistent vitreous opacities, vitreous hemorrhage, epiretinal membrane, macular hole and rarely retinal detachment [6, 7]. Data regarding the surgical management of retinal detachment in eyes with BD is sparse, and even more limited for combined rhegmatogenous retinal detachment and tractional retinal detachment (RRD/TRD) involving the macula [6, 8].
In this report, we describe successful management of an uncommon, severe case of combined RRD/TRD in a patient with severe ocular complications of BD. We detail the utilization of pars plana vitrectomy (PPV) without scleral buckling for the treatment of aggressive combined retinal detachment in this group of patients.
CASE REPORT
A 28-year-old Hispanic female presented with bilateral worsening vision of 1-week duration associated with history of recurrent oral and genital ulcers, as well as red, tender, nodular skin lesions over her extremities. Visual acuity (BCVA) upon presentation was 20/400 OD and light perception (LP) OS. Anterior segment examination was unremarkable. IOP was 16 mm Hg OD; 18 mm Hg OS.
Posterior segment examination revealed vitreous cells in the right eye, and mild vitreous debris in the left eye. Peripapillary hemorrhages, macular edema with associated retinal hemorrhages, vascular sheathing with areas of vascular occlusion, and patchy areas of retinal necrosis and intraretinal hemorrhages were noted in the fundus of both eyes (Fig. 1). Findings were more extensive in the left eye than the right, and consistent with hemorrhagic occlusive vasculitis with cystoid macular edema in both eyes.
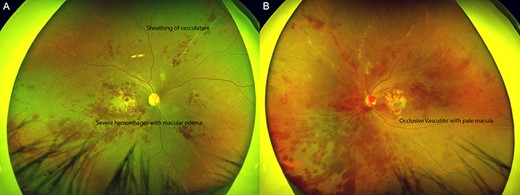
Hemorrhagic occlusive vasculitis in Behçet’s Disease. Wide angle fundus photos (Optos, Marlborough, MA) of the right (A) and left eye (B) demonstrating innumerable intraretinal hemorrhages concentrated in the macula and midperiphery, multiple sclerotic vessels and retinal soft exudates indicative ischemia, more prominent in the left than right eye.
Despite high suspicion for Behçet’s disease based on history and examination findings, the patient was admitted for further systemic evaluation. She underwent an anterior chamber paracentesis sampling of the aqueous for polymerase chain reaction (PCR) of Cytomegalovirus (CMV), Epstein–Barr Virus (EBV), Herpes Simplex Virus (HSV), Toxoplasma, and Varicella Zoster Virus (VZV), which were all negative. Serologies were obtained to evaluate for systemic inflammatory or underlying infectious etiologies including ANA, c-ANCA, p-ANCA, rheumatoid factor, HLA-B27, complement C3/C4, cryoglobulins, FTA-ABS, HIV, quantiferon gold, and immunoglobulin testing for VZV, HSV, Toxoplasma gondii, CMV, EBV, hepatitis panel, Coccidioides, also all negative. Human leukocyte antigen (HLA) testing revealed the patient was positive for HLA-B51/B5, and diagnosis of Behçet’s disease was made according to the clinical criteria established by the International Study Group for Behçet’s disease [2].
Additionally, biopsy of skin lesions demonstrated superficial and deep perivascular lymphohistiocytic inflammation with scattered neutrophils and leukocytoclastic debris, and focal septal panniculitis without fibrinoid necrosis of blood vessels, consistent with erythema nodosum. The patient was started on solumedrol 32 mg IV BID and azothiaprine 50 mg daily, and subsequently discharged on high-dose prednisone 60 mg PO daily and azathioprine 100 mg daily.
After hospital discharge, fluorescein angiography (FA) performed in the clinic demonstrated large areas of severe retinal nonperfusion (Fig. 2), retinal infarction and sheathed vessels with staining of vessel walls (typical of vasculitis). Ocular Coherence Tomography (OCT; Heidelberg Spectralis, Germany) demonstrated central foveal thickness (CFT) of 445 μm with subretinal fluid in the right eye, and a CFT of 779 μm with severe macular edema in the left eye. The patient received a subtenon kenalog 40 mg/cc injection in each eye.
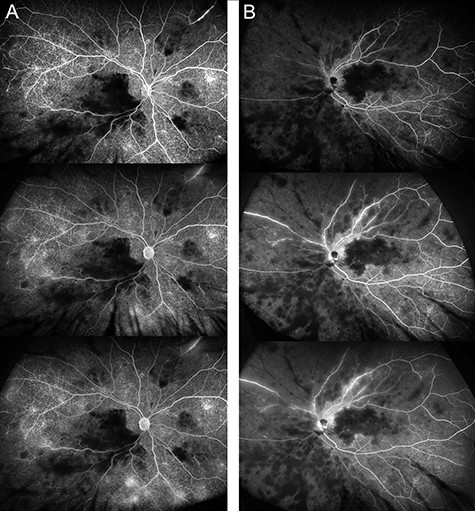
Severe retinal nonperfusion and infarction in Behçet’s Disease. Fluorescein angiography (FA) of right (A) and left eye (B) from early to late phase demonstrating areas consistent with severe retinal capillary nonperfusion and retinal infarction with persistent vasculitis more prominent in the left than right eye. Severe macular ischemia with enlarged FAZ secondary to occlusive vasculitis, a hallmark of Behcet’s disease.
Pan retinal photocoagulation (PRP) was performed to alleviate development of neovascularization from extensive retinal ischemia. Over the course of 1 month, she developed tractional fibrovascular membranes along the macula with a vitreous hemorrhage in the left eye. She received a series of three bimonthly intravitreal bevacizumab injections (1.25 mg/0.05 ml; Avastin Genentech, South San Francisco, CA). Despite aggressive interventions, retinal neovascularization progressed and she developed a complex combined RRD/TRD with proliferative vitreoretinopathy (PVR) in the left eye (Fig. 3A).
The patient underwent 3-port, small gauge (23 g) PPV with initial core vitrectomy followed by a peripheral vitrectomy to release traction over areas of retinal tears and detachment. Extensive bimanual dissection of tractional membranes was performed with drainage of subretinal fluid from pre-existing retinal breaks while performing a fluid-air exchange. Perfluorooctane was used to stabilize retina during dissection. Endolaser was then applied around retinal breaks, followed by 1000 centistoke silicone oil fill with successful reattachment of the retina (Fig. 3B). Despite complexity of the retinal detachment, scleral buckle placement was deferred in order to prevent potential exacerbation of ocular nonperfusion distal to buckle. Patient had uneventful postoperative recovery. BCVA improved from LP to counting fingers at 4 ft, 3 months after surgery.

Pre- and postoperative fundus photos of combined rhegmatogenous retinal detachment (RRD) and tractonal retinal detachment (TRD) with proliferative vitreoretinopathy in Behçet’s Disease. (A) Combined funnel RRD and TRD in the left eye. (B) Postpars plana vitrectomy, membrane peel and endolaser in the left eye with flat retina with laser scars one month after surgery. (C) Flat retina with laser scars 1 year after surgery; VA was 20/400.
One year after surgery, BCVA improved from LP to 20/400 in the left eye and retina remained flat (Fig. 3C). BCVA improvement was limited by extensive macular ischemia. The patient was eventually transitioned to adalimumab (intolerant to azothiaprine) coupled with a steroid taper. The patient continues to do well in the setting of collaborative management with dermatology, rheumatology and ophthalmology.
DISCUSSION
Vitreoretinal involvement in BD is associated with serious vision-threatening complications that may lead to irreversible vision loss. Although various posterior segment manifestations of BD have been cited in the literature, reports of retinal detachment and ensuing surgical outcomes in these patients remain sparse.
We present a case of a young woman with BD who developed an aggressive combined RRD and TRD with vitreous hemorrhage, which was successfully treated with PPV without scleral buckle.
Our findings are in concordance with a few reported cases [6, 8]. Mesquida et al., in a retrospective review, reported three eyes with retinal detachments managed with PPV in patients with vitreoretinal complications of Behçet’s-associated uveitis. One patient of the three had a peripheral, macula-sparing combined RRD/TRD with vitreous hemorrhage. This patient underwent 3-port 20-gauge PPV with the use of SF6 instead of silicone oil (as was used in our patient) [6].
A study by Dabour et al. reported successful repair with PPV for a macula-involving combined RRD/TRD secondary to an old branch retinal vein occlusion in a patient with BD. Interestingly, this patient had a prior history of intravitreal triamcinolone acetonide injection, which was postulated as a possible risk factor for retinal detachment [8, 9]. Macular hole with retinal detachment in BD has also been reported with successful repair with standard 20-gauge vitrectomy with peeling of the internal limiting membrane and retinal tamponade with either SF6 or silicone oil [6, 10]. Additionally, there have been reports of exudative retinal detachment with necrotizing retinitis during the course of BD. These patients were managed nonsurgically with aggressive steroid therapy and long-term administration of immunomodulatory agents in view of exudative nature.
As noted in our patient, combined forms of severe total retinal detachment can occur in the setting of BD. This pathology is likely sourced from a complex cascade of retinal vaso-occlusion, consequential tissue hypoxia and associated increased vascular endothelial growth factor (VEGF) expression [1]. In this setting, VEGF is a key player in the propagation of retinal neovascularization, vitreous hemorrhage and formation of fibrovascular membranes, which lead to retinal detachment. Additionally posterior uveitis may facilitate retinal tear formation and subsequent RRD due to peripheral vitreoretinal traction [8, 9]. It is likely that these pathophysiologic processes explain our patient’s severe form of vitreoretinal involvement, ultimately, resulting in combined RRD/TRD with vitreous hemorrhage. It is noteworthy that anti-VEGF agents had limited effect on the progress of the disease.
BD is more common in males, in patients of Middle Eastern or Japanese descent, and male gender is typically associated with worse visual outcomes compared to females. Our patient is unique as she is Hispanic with a severe form of the disease. Despite normal anatomical recovery, improvement in visual acuity is limited due to extensive retinal ischemia in our patient. Despite intravitreal anti-VEGF therapy, PRP and aggressive systemic immunosuppressive therapy, patient still developed severe combined retinal detachment (Fig. 3A). Encouragingly, PPV, complete membrane removal and endolaser without scleral buckling achieved anatomic success (Fig. 3C) and improved visual acuity. A scleral buckle was not utilized in our patient as it may have further compromised peripheral perfusion, exacerbating already existing nonperfusion.
In summary, we describe successful management of combined RRD/TRD, a rare, sight-threatening posterior segment complication of BD with PPV. A year after surgical intervention, retinal detachment has completely resolved and visual acuity improved despite severe macular ischemia. PPV without scleral buckling can serve as an effective surgical option to achieve favorable visual and anatomic outcomes in these patients.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}