





Abstract
Primary retroperitoneal teratomas involving adrenal glands are extremely uncommon, particularly in elderly males. Only a few case reports have been documented in the literature so far. We report a mature cystic retroperitoneal teratoma in the region of left adrenal gland in an asymptomatic 75-year-old male patient. It was incidentally found on an abdominal computed tomography scan and was thought to be an adrenal adenoma. Because of its relatively large size and the patient’s request, he underwent a laparoscopic left adrenalectomy. Histopathological examination revealed a benign mature cystic retroperitoneal teratoma in the region of the left adrenal gland. The patient had an uneventful postoperative course and is free of recurrence after 20 months of follow-up. Considering the diagnostic difficulty of retroperitoneal teratoma by radiologic imaging, and its risk of malignancy, surgical resection via a minimally invasive approach would be the best diagnostic and therapeutic option. A literature review on teratomas is included.
INTRODUCTION
Primary mature teratomas are rare nonseminomatous germ cell tumours, composed of well-differentiated parenchymal tissues that are derived from at least two of the three germ cell layers [1]. They typically occur in midline (paraxial) structures, mainly within the gonads [1, 2]. The extragonadal sites (intracranial, cervical, mediastinal, retroperitoneal and sacrococcygeal regions) account for 15% of all teratomas, and the retroperitoneum is the least common site [2]. As gonadal malignancies commonly metastasize to the retroperitoneum it is important to differentiate true primary retroperitoneal neoplasms [3]. Primary retroperitoneal teratomas involving adrenal glands are extremely rare accounting for <4% of all primary teratomas [1, 2]. Cases are reported usually in infancy or in young females, mainly in the sacrococcygeal area, but are extremely infrequent in adults [3]. The majority of cases is asymptomatic, present with vague symptoms or are identified incidentally on routine investigations [3, 4]. Surgical excision of mature teratoma remains the mainstay of treatment and is required for a definitive diagnosis [3, 4].
The aim of this article is to present a rare case of a retroperitoneal mature cystic teratoma involving the left adrenal gland in an asymptomatic 75-year-old male patient, who was referred for evaluation of an adrenal incidentaloma and underwent a laparoscopic adrenalectomy. The present case emphasizes limitations of image-based diagnosis of adrenal masses and also the diagnostic and therapeutic role of minimally invasive surgery for them.
CASE REPORT
An asymptomatic 75-year-old Caucasian male was referred to our institution for the evaluation of an incidental left adrenal mass pointed out on computed tomography (CT) scan at medical checkup. The patient had a past medical history of hypertension and benign prostatic hyperplasia. The medication list included perindopril, indapamide, bisoprolol and tamsulosin. He had no previous surgeries and his family history was unremarkable. Physical examination was normal. Abdominal contrast-enhanced CT scan revealed a 5.6 × 3.5 × 3 cm, solid, nodular, hypodense mass that was thought to be arising from the left adrenal gland, suggesting an adenoma (Figs 1 and 2).
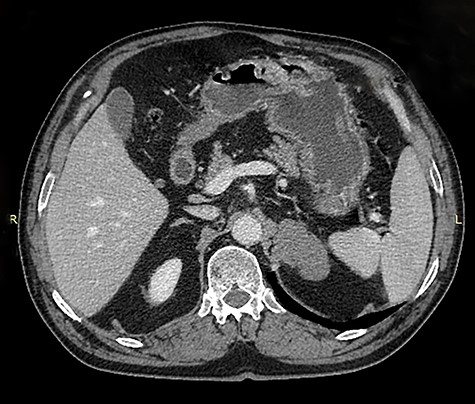
Axial image of contrast enhanced computed tomography of abdomen showing a mass that was thought to be arising from the left adrenal gland.

Coronal image of contrast enhanced computed tomography of abdomen and pelvis showing a hypodense mass in the region of the left adrenal gland, medial to the spleen and above the kidney.
Laboratory studies to exclude a functioning adrenal tumour and tumour markers (CA19.9, CEA, PSA, alpha-fetoprotein (AFP), human chorionic gonadotropin (hCG)) were normal.
Because of its relatively large size and the patient’s request, he underwent a laparoscopic transperitoneal left adrenalectomy in the right lateral decubitus position (two 10-mm and one 5-mm ports). Intraoperatively, an enlarged left adrenal gland and a cystic lesion closely adherent to it were found, surrounded by adipose tissue (Figs 3 and 4). They were completely resected en bloc and removed in the endobag. No adverse events occurred postoperatively and he was discharged on Day 3.
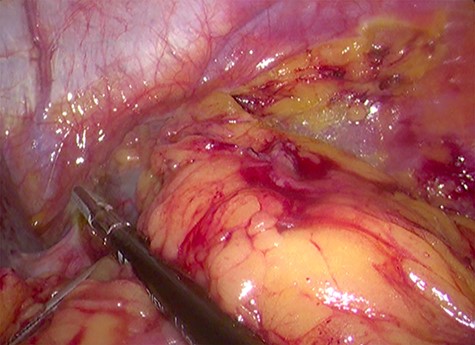
Laparoscopic view of the retroperitoneal space containing the left adrenal gland and a cystic lesion surrounded by large amounts of adipose tissue.
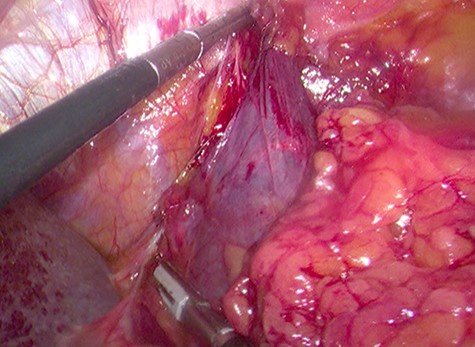
Laparoscopic en bloc resection of the retroperitoneal cystic lesion adherent to the left adrenal gland and adipose tissue.
Macroscopically, the specimen consisted of a walled cyst filled with yellowish greasy material measuring 4.5 × 3.5 × 2cm and the left adrenal gland measuring 5 × 3 × 2 cm, both surrounded by adipose tissue. Microscopic evaluation revealed a mature cystic teratoma and a left adrenal gland without morphologic changes (Fig. 5). Neither immature nor malignant components were identified. After 20 months of follow-up, he is free of recurrence.
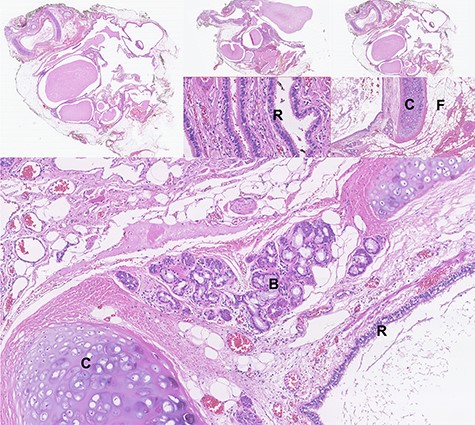
Photomicrographs of haematoxylin-eosin stained tissue sections showing the microscopic features of the mature cystic teratoma: cystic spaces lined with respiratory epithelium (R), areas of cartilage (C) with mucinous- and serous-type bronchial glands (B), abundant fibroadipose tissue (F), lymphoid structures, smooth muscle, nerve and ganglionic tissue.
DISCUSSION
A retroperitoneal mature cystic teratoma in the region of the left adrenal gland in a 75-year-old man is a very rare event and only a few cases have been reported in the literature [3]. Teratomas are classified as (i) mature, when they contain differentiated tissue, (ii) immature, when they have predominantly embryonic or undifferentiated tissue, (iii) teratoma with malignant transformation and (iv) monodermal, when there is a predominance of tissue arising from one germ cell layer [2, 3]. The mature cystic teratoma is a congenital tumour developed from pluripotent embryonal cells [1]. Although it mainly occurs in the ovaries and testes, teratomas can occur in almost any region of the body [1]. Retroperitoneal teratomas account for 1–11% of all primary retroperitoneal neoplasms, being more common in the first 6 months of life and in early adulthood [3, 5]. Like in the presented case, retroperitoneal teratomas are commonly found at the left side of the body, above the upper pole of the kidney [3], and they are usually asymptomatic or present with non-specific complaints, making it difficult to diagnose preoperatively.
This case report emphasizes that these tumours should be considered in differential diagnosis of an adrenal incidentaloma, as a radiographic evaluation did not confirm the origin of the retroperitoneal mass. Serum markers, such as CA19.9, CEA, and AFP, can be elevated in retroperitoneal teratomas [6]. These markers were checked in the presented patient before the surgery, allowing for monitoring a successful treatment or relapse of the tumour.
Radiographic evaluations play valuable roles in diagnosis and planning the surgical treatment of teratomas. Ultrasound can differentiate between cystic and solid elements and CT scan can better distinguish between fat and calcified masses [6, 7]. Nevertheless, magnetic resonance imaging scans can provide better resolution of the soft tissues, feasible identification of benign and malignant features and has superior tumour staging assessment [6, 7].
Surgical excision of the tumour is required for a definitive diagnosis (by histopathological examination) and remains the main treatment option [3, 4]. Prognosis is excellent after complete surgical excision with an overall five-year survival rate of nearly 100% [8]. These neoplasms are greatly resistant to radio- and chemotherapy and these treatments are used for teratomas with malignant features [3]. Nowadays, minimally invasive surgery using a laparoscopic approach (transperitoneal or retroperitoneal) is becoming a more frequent procedure, leading to an earlier recovery and less morbidity than conventional open surgery [4, 9].
Malignancy rate of retroperitoneal teratomas in adults is significantly higher than in children (26% vs. 7%) [3]. The pathological criteria for benign lesion are (i) absence of malignant or immature elements in the tumour, (ii) absence of other similar lesions in other parts of the body, (iii) normal levels of AFP and hCG and (iv) absence of recurrence on follow-up [4]. Despite the benign nature of mature cystic teratoma, close follow-up is recommended because the incidence of malignant transformation is ~3-6% [4]. Our patient is free of recurrence and metastasis within 20 months post-surgery and is completely asymptomatic.
In conclusion, primary retroperitoneal teratomas in older males involving the region of adrenal gland is extremely rare and should be included in the differential diagnosis of non-functioning adrenal incidentalomas. A minimally invasive approach can be done safely with improved outcomes.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}