





Abstract
Sarcomatoid malignant peritoneal mesothelioma is the rarest and most lethal form of peritoneal mesothelioma. We present the case of a sarcomatoid malignant peritoneal mesothelioma presenting as a localized mesenteric tumor in a 54-year-old female with no previous asbestos exposure. This clinical presentation is extremely rare and is the first documented in Cameroon.
INTRODUCTION
Malignant mesothelioma is a rare and aggressive neoplasm arising from serous surfaces [1, 2]. As the second most frequent site after the pleura (65–70%), peritoneal mesothelioma has an incidence of one per million and accounts for 10–30% of all mesotheliomas [1]. From three basic histologic forms of malignant peritoneal mesothelioma, sarcomatoid mesothelioma is the rarest form [2, 3], and the most serious of all asbestos-related diseases [4]. We present the case of a sarcomatoid malignant peritoneal mesothelioma presenting as a localized mesenteric tumor in a 54-year-old female with no previous asbestos exposure. This clinical presentation is extremely rare and is the first documented in Cameroon.
CASE REPORT
A 54-year-old female was admitted with a 6-month history of a painless abdominal mass, gradually increasing in size. She was a lifelong teacher in secondary school and has lived in one area for a lifetime, there was no asbestos-related facility. She had never been exposed to asbestos and had received an appendectomy and caesarean section, respectively, 8 and 15 years ago. She was not smoking, and her family history was negative for malignancy. On admission, she looked in a good health state, her vital signs were stable, and a movable and painless intracavitary mass was palpable over the right side of the abdomen, but ascites signs were absent. The blood count showed a white cells count of 13.100/mm3 (neutrophils 70.2%, lymphocytes 39.6%), haemoglobin of 12.4 g/dl, and platelets count of 200.000/mm3. The blood chemistry showed a creatinine level of 10 mg/l, urea 0.11 g/l and CRP < 6 mg/dl. As a result of the abdominal computed tomography scan was not sufficiently conclusive on the nature of the mass, the surgical team decided to perform an exploratory laparotomy. Laparotomy showed a localized mesenteric encapsulated and firm tissue mass weighing ~500 grams and measuring 12.5 × 10.5 × 8 cm, with no evidence of inflammation, mesenteric lymph nodes and ascites (Fig. 1). Microscopically, the tumor consisted of moderately polymorphic spindle-shaped neoplastic cells with elongated moderately pleomorphic hyperchromatic nuclei, with low mitotic activity and infiltrating connective tissue (Fig. 2). These histopathological features were compatible with a low grade sarcomatoid malignant mesothelioma. The neoplasic cells were positive with keratin AE1/AE3, CAM 5.2, and negative for desmin and CD34, which was consistent with the diagnosis. The patient has been referred to oncologist, and adjuvant chemotherapy protocol has been planned.

Well defined lobulated and encapsulated mass weighing ~500 g and measuring 12.5 × 10.5 × 8 cm dimensions.
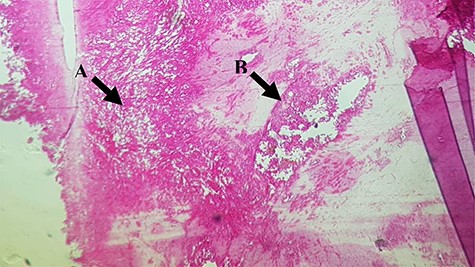
(A) Moderately polymorphic spindle-shaped cells with elongated moderately pleomorphic and hyperchromatic nuclei and low mitotic activity; (B) Note some layers of atypical mesothelial cells.
DISCUSSION
Malignant peritoneal mesothelioma is a fatal, treatment-resistant, and asbestos-related neoplasm of the serosal lining of the peritoneum, with an incidence of one per million [5]. According to epidemiological data, the overall incidence of this disease is higher in males than in females, which can be interpreted by more chances of occupational and environmental asbestos contact in men [2, 5]. In this case, the patient was a female with no previous exposure to asbestos. However, exposures to radiation, talc, mica, erionite, thorotrast, Hodgkin’s disease, and viral infections have also been reported to be correlated with malignant peritoneal mesothelioma [5]. Although malignant peritoneal mesothelioma can occur in any age group, in most series, the age of affected patients varies from 49 to 84 years old [1, 2, 4, 6, 7], which is concordant to our patient age (54 years old).
Although the main risk factor of malignant peritoneal mesothelioma according to the literature is asbestos exposure, no asbestos exposure is documented in about 20–40% of patients [2, 3], and it is the case of our patient who has never been exposed to asbestos.
According to the literature, there are no specific symptoms and clinical features in malignant peritoneal mesothelioma. Therefore, the preoperative diagnosis is difficult and misdiagnosis can happen [3]. Indeed, Saisho et al. [6] reported a case of localized biphasic malignant mesothelioma presenting as a rectal tumor with a complaint of anal bleeding, Naraynsingh et al. [7] reported a case of a malignant mesothelioma presenting as a recurrent adhesion obstruction and Frontario et al. [8] reported a primary peritoneal mesothelioma resulting in small bowel obstruction. In our case, the patient was admitted with a 6-month history of painless abdominal mass, gradually increasing in size without any associated signs. This clinical presentation is no common in literature as an initial complaint in the case of peritoneal mesothelioma. Indeed, the most common presentations reported in series are abdominal distension and pain caused by the accumulation of ascites and tumors, ranging 41–86 and 31–87%, respectively. The less common initial complaints including weight loss, abdominal mass, fever, diarrhea, vomiting, and the new-onset hernia can be seen in 32, 30, 22, 17, 15 and 12% patients [1, 4, 5]. Additionally, the clinical presentation with intestinal obstruction, hypercoagulability, thrombocytosis with anemia or surgical emergency (due to acute inflammatory lesions) has been also reported [2, 3, 7–9].
The diagnosis of mesenteric tumor was made by exploratory laparotomy. This invasive diagnostic procedure is comparable to those performed in other settings. Indeed, Saisho et al. [6] reported that laparotomy or laparoscopy with biopsy was required to make the definitive diagnosis in 96% of cases to make a diagnosis of malignant peritoneal mesothelioma. In the Washington Cancer Institute series, diagnosis was obtained by laparotomy in 44% of patients [3].
In many reported cases, malignant peritoneal mesothelioma appeared at laparotomy as a widespread nodular thickening of the visceral peritoneum with a striking, diffusely uniform, erythematous appearance or omental cake with peritoneal nodular seed with the presence of ascites [1, 4, 7]. In our case, it was different with a gross appearance of a localized mesenteric encapsulated tissue mass weighing ~500 g and measuring 12.5 × 10.5 × 8 cm, with no inflammation, mesenteric lymph nodes and ascites. Note that localized form of malignant peritoneal mesothelioma is very rare, representing about 2% of macroscopic presentations of this neoplasm [6]. In the case reported by Saisho et al. [6] of localized biphasic malignant mesothelioma presenting as a rectal tumor, the neoplasm measured 8 cm of maximal diameter, which is comparable in size to the mesenteric tumor of our patient.
In histopathology examination, this mesenteric tumor consisted of moderately polymorphic spindle-shaped neoplastic cells with elongated moderately pleomorphic hyperchromatic nuclei, with mitotic activity and infiltrating connective tissue. This description is concordant with histological description of a sarcomatoid malignant peritoneal mesothelioma in the literature [4, 5]. According to literature, mesotheliomas have three basic histologic forms: epithelioid (the most frequent), sarcomatoid or mixed (biphasic) [1, 3, 5–7]. More often, areas showing features and admixtures of these three types may be encountered within a single tumor; a sarcomatoid component is observed in 25% of cases, but a pure sarcomatoid variety is extremely rare and only 32 cases have been reported in the literature since 2006 [2, 9]. Sarcomatoid mesothelioma is extremely rare: Deraco et al. [3] in a series of 49 malignant peritoneal mesothelioma reported no sarcomatoid histotypes. The immunohistopathological findings from our case were consistent with the diagnosis of sarcomatoid mesothelioma, as described by some authors [10].
The 2006 Milan Consensus Conference on Peritoneal Surface Malignancies concluded that the standard treatment of malignant peritoneal mesothelioma is based on the integration of is cytoreduction surgery and hyperthermic intraperitoneal chemotherapy [2, 3, 6, 7, 9]. For this reason, after the diagnostic confirmed by histopathology examination, the patient has been referred to oncologist for adjuvant chemotherapy.
Due to the rarity of malignant peritoneal mesothelioma and variable treatment strategies, prognostic factors had not been well identified in the past century [5]. However, a combined treatment of surgery and adjuvant chemotherapy has been demonstrated to be correlated with a promising improved survival compared with traditional therapies and female gender has been previously demonstrated to be a favorable prognostic factor of malignant peritoneal mesothelioma [5]. Based on this evidence, we can expect a good prognosis for our patients.
In conclusion, we presented the case of a sarcomatoid malignant peritoneal mesothelioma presenting as a localized mesenteric tumor in a 54-year-old female with no previous asbestos exposure. The interests of reporting this case were that: firstly, the sarcomatoid histological type of this neoplasm is very rare and the patient had an uncommon clinical presentation with a painless abdominal mass as a single symptom. Secondly, localized form of peritoneal mesothelioma as a single tumor accounts for about 2% of macroscopic presentation and the mesenteric site is exceptional making diagnostic to be a challenge for physicians. Additionally, the authors think about either genetic or viral origins of the neoplasm. We, therefore, recommend to consider the differential diagnosis of malignant peritoneal mesothelioma in patients with an abdominal mass.
ACKNOWLEDGEMENT
We thank the nurse staff of the Mbouo Protestant Hospital’s Surgery Department for their contribution in the management of the patient.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}