





Abstract
Gallbladder volvulus is a rare condition with similar presentation to acute cholecystitis. It is caused by the gallbladder twisting upon its mesentery leading to potential ischemia and biliary obstruction. A 77-year-old female presented with symptoms of right upper quadrant pain and nausea. She was found to have an elevated leukocytosis and a palpable right upper quadrant abdominal mass on exam. Imaging revealed a severely distended gallbladder with pericholecystic fluid and wall thickening without gallstones. Intraoperatively, an extremely distended, ischemic gallbladder was noted to have twisted upon its mesentery. The structures were able to be identified and the gallbladder was able to be safely removed with a laparoscopic approach despite its large size. Gallbladder volvulus is important to consider in the differential of acute cholecystitis because delay in intervention could lead to gallbladder necrosis and possible perforation, increasing the patient’s morbidity and mortality.
INTRODUCTION
Gallbladder volvulus is an uncommon disease caused by torsion of the gallbladder around its mesentery along the axis of the cystic duct and artery, ultimately leading to gallbladder ischemia and obstruction of biliary drainage. This diagnosis was first discovered in 1898 by an American surgeon Wendel, who referred to the condition as ‘floating gallbladder [1–3].’ Gallbladder volvulus only accounts for 1 out of 365,000 cases of gallbladder disease [2, 3]. Laparoscopic cholecystectomies are one of the most common surgical procedures performed in the United States and, although rare, it is important for surgeons to familiarize themselves with this condition due to its severe complications.
CASE REPORT
A 77-year-old female presented with acute right upper quadrant (RUQ) pain with associated nausea for 12 hours. Pain was described as dull and more severe after eating. The patient had prior episodes of this pain, occurring for the last several years. She admitted weight loss and denied any fevers, chills or vomiting. Medical history included hypothyroidism, hyperlipidemia, malabsorption problem for which she takes B12 and folic acid supplements. Surgical history included appendectomy. She denied any tobacco or alcohol use. Abdominal exam demonstrated a soft, non-distended abdomen with a palpable mass in the RUQ, RUQ tenderness to palpation without rebound or guarding. Lab values were significant for an elevated leukocytosis; chemistry and hepatic function panel within normal limits. CT scan demonstrated a distended hydropic appearing gallbladder with pericholecystic fluid and wall edema without evidence of gallstones (Fig. 1) and a common bile duct of 9 mm. Subsequent RUQ ultrasound revealed a dilated gallbladder with a thickened wall and a small amount of pericholecystic fluid, suggestive of acalculus cholecystitis. The patient was admitted, started on Cefepime and Flagyl, and scheduled for a laparoscopic cholecystectomy. Upon entering the abdomen, a large necrotic, gangrenous appearing gallbladder was noted (Fig. 2a–d). It had maneuvered itself over the top of the liver and completely necrosed its base. The gallbladder was extremely distended, encompassing much of the patient’s RUQ. The common bile duct was able to be identified. The gallbladder was not detorsed due to risk of toxin release into circulation as the gallbladder was gangrenous. Decompression of the gallbladder was not attempted due to concern for a possible malignancy. A 12 mm trocar was placed in the RLQ and a GIA stapler with Peristrips was used to completely transect the base of the gallbladder, including the cystic artery and duct. The gallbladder was placed in a large EndoCatch bag and the umbilical incision was extended to remove it from the abdomen. Hemostasis was achieved at the staple line and no other evidence of abnormalities were noted. The patient tolerated the procedure well. The patient had an uncomplicated postoperative course. Her postoperative hepatic function panel remained within normal limits. Histopathology was consistent with acute cholecystitis with gallbladder hemorrhage and necrosis (Fig. 3).

CT scan demonstrating a distended hydropic appearing gallbladder with pericholecystic fluid and wall thickening.
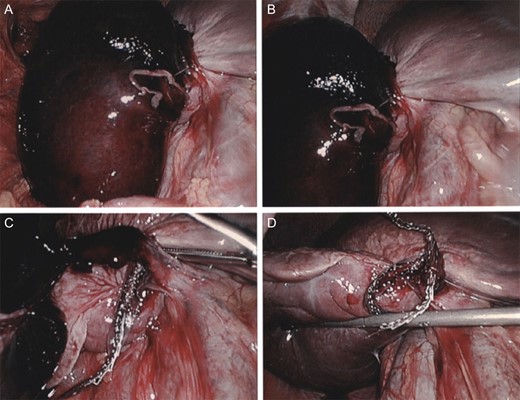
(a) Initial laparoscopic view of a severely distended and displaced gallbladder encompassing much of the RUQ. (b) Gallbladder base appears to have twisted upon itself and necrosed the base. (c) Transection across the gallbladder base with a GIA stapler. (d) Hemostasis achieved at transection size without damage to the liver.
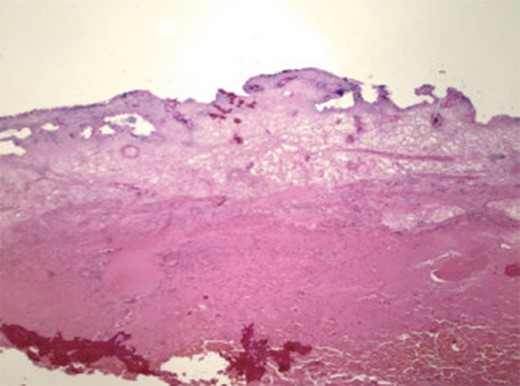
Histopathology revealed acute cholecystitis with hemorrhage and necrosis of the gallbladder.
DISCUSSION
Gallbladder volvulus, or torsion, is a rare cause of acute RUQ pain. The etiology of the condition is unknown. Hypothesized contributory factors include anatomical abnormalities including a long gallbladder mesentery allowing it to float freely from the liver bed and easily twist upon itself [2, 3]. Volvulus is more common in elderly females in the seventh and eighth decades of life [2, 3]. It is likely due to loss of visceral fat with aging. A ‘triad of triads’ has been described for this condition, including appearance (elderly, thin, spinal deformities), symptoms (sudden onset, RUQ pain, early emesis) and examination (non-toxic, palpable mass, pulse-temperature discrepancy) [2–5]. Imaging can show the gallbladder out of its typical fossa which can increase one’s index of suspicion, however, usually it is nonspecific and similar to that seen in acute cholecystitis. Cholelithiasis is only present in about 24% of patients [2, 3]. Gallbladder volvulus is often misdiagnosed. Knowledge of the condition’s typical radiographic and clinical findings can help prompt surgeons to proceed with immediate surgical intervention. Volvulus can usually be treated with a laparoscopic approach. According to literature, the principles to the procedure include decompression, detorsion, and cholecystectomy [3]. However, we do not fully agree with this as it has been shown that detorsion in the state of necrosis can lead to toxin release secondary to reperfusion ultimately leading to systemic effects. Torsion has been noted to occur both clockwise and counterclockwise, related to gastric or colonic peristalsis respectively [2, 3]. Delayed intervention can lead to gallbladder necrosis, which can be complicated by perforation, bilious peritonitis and hemodynamic instability [2]. Hence, gallbladder volvulus is important to include in the differential diagnosis of acute RUQ pain as delayed intervention may mandate open cholecystectomy, increasing morbidity and mortality.
In conclusion, gallbladder volvulus is an uncommon surgical emergency. Pre-operative diagnosis is rare; however, a high suspicion should prompt urgent surgical intervention. Intraoperative decision making plays a crucial role in this condition in order to proceed with the procedure safely and without increasing morbidity and mortality.
ACKNOWLEDGMENTS
No acknowledgments or non-financial support.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}