





Abstract
A 36-year-old morbidly obese female with BMI 66 kg/m2, scheduled for elective laparoscopic sleeve gastrectomy. Prior to the surgery patient had symptoms of mild dyspnea, vague abdominal discomfort. CAT scan of thorax and abdomen revealed a right-sided large morgagni diaphragmatic hernia containing omentum and portion of the transverse colon. Patient elected to undergo Laparoscopic sleeve gastrectomy and concomitant morgagni diaphragmatic hernia repair. The post-operative course was uneventful and the patient was discharged on post-operative Day 2.
This case is an extremely rare case of super obese patient with Morgagni hernia who desires bariatric surgery and found to have incidental finding of morgagni hernia. This kind of combination can safely undergo concomitant laparoscopic hernia repair with mesh and sleeve gastrectomy.
INTRODUCTION
Morgagni hernias are one of the congenital diaphragmatic hernias. Diaphragmatic hernias of Morgagni were first described by the Italian anatomists and pathologist Giovanni Battista Morgagni in 1769 [1]. They are rarest of congenital diaphragmatic hernias, making up 2–3% of cases [2]. Hernia of Morgagni is located just posterolateral to the sternum. It has also been called retrosternal, parasternal, substernal and subcostosternal. It can occur on either side of the sternum through a muscle free triangular space called the Larrey space, although it is more common on the right side [3]. The majority of hernias of Morgagni are diagnosed late because patients can be asymptomatic or present with non specific respiratory or gastrointestinal symptoms and signs. They may also be associated with trauma, surgery and increased intrabdominal pressure and have been known to contain omentum, stomach, transverse colon and even liver [4]. It is diagnosed with a lateral chest radiograph and confirmed with a barium enema or computed tomogram. Although the majority of these hernias are asymptomatic, repair is recommended to avoid future complications.
CASE DESCRIPTION
We report a 36-year-old morbidly super obese female with BMI 66 kg/m2, came to the obesity center at Dr. Suliman Alhabib hospital, Altakhasusi branch and scheduled for elective laparoscopic sleeve gastrectomy.
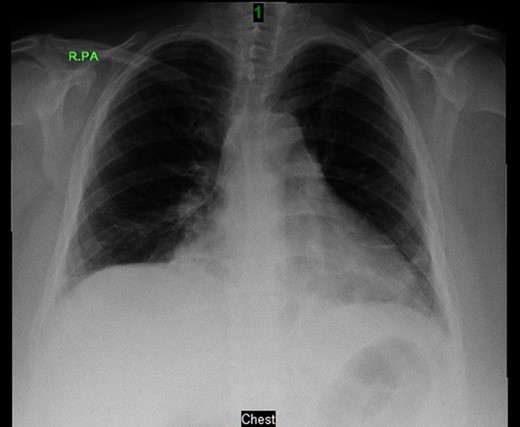
Prior to the surgery patient had symptoms of mild dyspnea, vague abdominal discomfort and an initial evaluation with Chest X Ray revealed bowel gas pattern in the right hemithorax (Fig. 1). A subsequent CAT scan thorax and abdomen revealed a right-sided large morgagni diaphragmatic hernia containing omentum and portion of the transverse colon (Fig. 2). Patient elected to undergo Laparoscopic sleeve gastrectomy and concomitant morgagni diaphragmatic hernia repair. Abdomen was explored laparoscopically which revealed a right sided morgagni diaphragmatic hernia with defect size about 8 × 4 cm, containing omentum, transverse colon and part of the falciform ligament. Contents were reduced successfully taking care not to injure the bowel, falciform ligament partially dissected. A sleeve gastrectomy done. Then the hernial defect was closed primarily by interrupted non absorbable sutures. The closure was then reinforced with a sublay ventralight mesh which was secured using transfascial fixation sutures and with tackers (Fig. 3). The post operative course was unremarkable and the patient was discharged on post operative Day 2 with normal chest X-ray (Fig. 4). At 2 months after surgery the patient was doing well and tolerating solid and liquid diet and no more dyspnea nor GI symptoms.
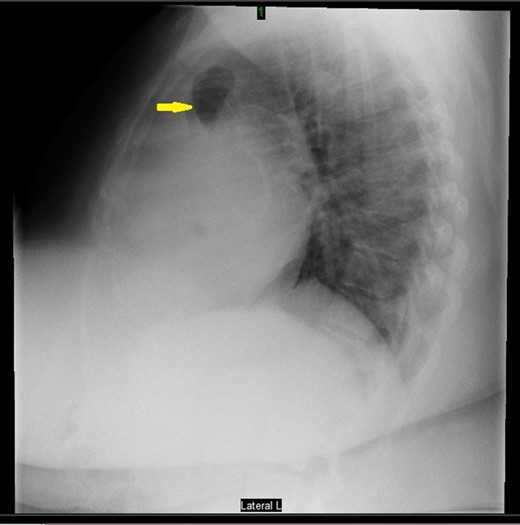
Preoperative chest X-ray revealed bowel gas.

CAT scan thorax and abdomen revealed a right-sided large morgagni diaphragmatic hernia.

Laparoscopic sleeve gastrectomy with concomitant Morgagni hernia repair.
Post-operative chest X-ray.
DISCUSSION
All symptomatic as well as asymptomatic Morgagni Hernias should be repaired to avoid complications, laparoscopy is the safest approach in asymptomatic cases.
Simultaneous laparoscopic repair of morgagni hernia and sleeve gastrectomy in morbidly super obese patients is safe and effective. The procedure is well tolerated, feasible and can reduce the cost of multiple hospital admissions.
The case presented highlights the safety of concurrent Morgagni hernia repair and bariatric surgery. Up to our knowledge from the literature review this is the first case to be reported as morbidly super obese patient underwent concurrent Morgagni hernia repair along with sleeve gastrectomy.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}