





Abstract
A 53-year-old man with previous history of sigmoid colon adenocarcinoma who had undergone surgical resection and adjuvant chemotherapy presented with slightly rising carcinoembryonic antigen (CEA), while anatomical imaging modalities were unremarkable. FDG PET-CT study did not identify residual tumoral disease; however, there were abnormalities in the gallbladder most likely suggestive of cholecystitis. Eight weeks after cholecystectomy, serum CEA concentration reached normal values. Final histopathology of the gallbladder was also consistent with acute on chronic cholecystitis.
BACKGROUND
Recommended methods for periodic surveillance of patients with colorectal cancer include clinical assessment, measuring serum carcinoembryonic antigen (CEA), chest and abdominopelvic computed tomography and repeated colonoscopy [1]. These methods all have their advantages and limitations. Elevated serum CEA is not highly specific for colon cancer recurrence, while various other gastrointestinal disorders such as pancreatitis, peptic ulcer disease, biliary tract abnormalities (benign or malignant) and liver disorders may contribute to increased serum CEA and false-positive results [2]. The other main limitation of tumor markers is their failure to localize the lesions, highlighting the necessity of imaging modalities during colon cancer assessment and surveillance (i.e. ultrasonography, computed tomography, magnetic resonance imaging, positron emission tomography, etc.) [3]. Nowadays, FDG PET-CT is recommended as a useful tool for restaging patients with colorectal cancer, considering its usefulness in differentiating benign and malignant lesion [4, 5]. On the other hand, regarding the mechanisms involved in FDG distribution, a potential important pitfall of FDG PET is the false-positive results due to abnormal increased FDG accumulation in inflammatory lesions [6]. Here we present a case of previous colon cancer who was thought to have a recurrent/metastatic disease, according to his elevated serum tumor marker, but further investigation by FDG PET/CT found that rising serum CEA was a false-positive finding originating from gallbladder inflammation. The pattern noticed in the gallbladder on FDG PET-CT study was interpreted as cholecystitis which was confirmed later by histopathology.
CASE PRESENTATION
A 53 years old man with a history of large bowel obstruction secondary to a sigmoid mass had undergone urgent sigmoid resection and colon anastomosis about 12 months earlier. Histopathologic survey demonstrated sigmoid adenocarcinoma. Thus, he received eight courses of adjuvant chemotherapy. Tumor marker was within the normal range at the end of treatments. During surveillance, carcinoembryionic antigen (CEA) level slightly elevated along with new symptoms of upper abdominal pain; although CT imaging from the chest, abdomen and pelvis revealed no remarkable abnormal finding except a small gall stone. The patient was referred for FDG PET-CT to detect possible recurrence or metastasis. On FDG PET-CT study, no clear evidence in favor of residual or metastatic disease was identified; however, the gallbladder was distended and located in an unusual position. The gallbladder contained small stones accompanied with mural calcification in the neck. Gallbladder wall thickening was also seen demonstrating a ring like pattern of increased FDG uptake with SUVmax = 6.5. These findings were interpreted as acute/chronic cholecystitis (Fig. 1). On the basis of this interpretation, the patient was referred back for cholecystectomy. After the operation, he was clinically improved and 8 weeks later the serum CEA level came back to normal range. Histopathologic examination was compatible with acute on chronic cholecystitis confirming FDG PET-CT result. In long-term follow up, CEA is within normal values with no evidence of recurrence till February 2019 (Table 1).
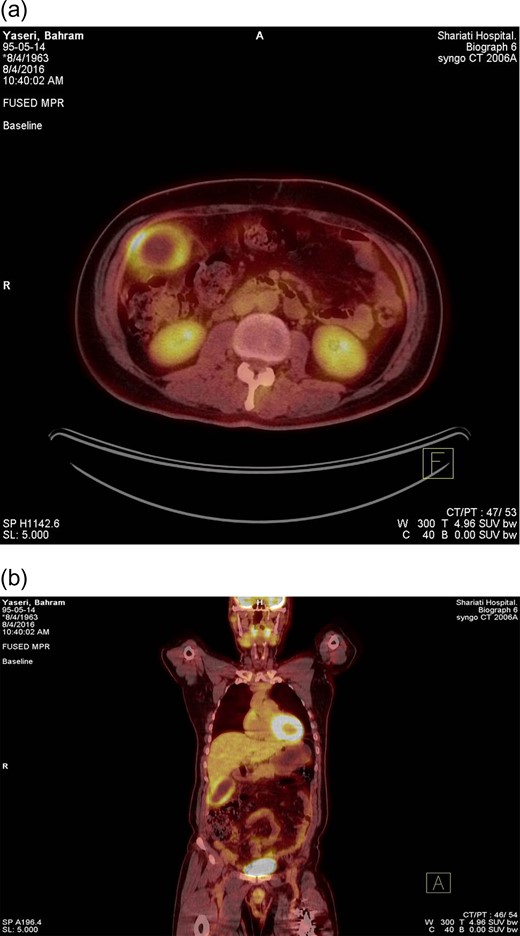
FDG PET-CT with (a) trans-axial and (b) coronal views. PET-CT scan performed to evaluate a patient with colon cancer interfacing mild rise in blood CEA level. One hour after the intravenous administration of 11 mCi of 18 F-FDG, PET-CT images were obtained. A strikingly enlarged gallbladder shows intense radiotracer uptake in the gallbladder wall with a central photopenic area representing a rim like pattern. Metabolically active wall proposes the possibility of cholecystitis (acute/chronic). The patient underwent laparoscopic cholecystectomy. The histopathologic evaluation confirmed imaging findings as acute on chronic cholecystitis. Two months following surgical intervention, the CEA level declined to the normal range.
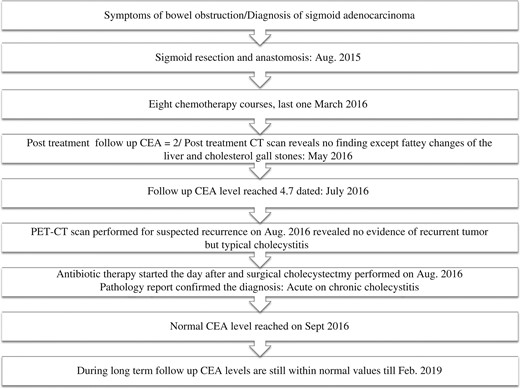
Schematic presentation of disease course, therapeutic interventions and CEA levels.
 |
DISCUSSION
Increased serum CEA level, secondary to biliary tract diseases, such as obstruction, inflammation and epithelial malignancies of bile ducts has been already reported [7–9]. Elevated tumor markers, either CEA or CA19-9, are not specific in gallbladder malignancies and have both been identified in xanthogranulomatous cholecystitis (XGC) as well as gallbladder cancer (GC) [7]. Also extrahepatic biliary tract obstruction including cholangitis and common bile duct (CBD) stone are accused to cause high CEA values, even more than cholecystitis and gallbladder stone. Serum CEA level returned to normal after relief of the obstruction [8].
Ring-like FDG uptake were previously mentioned in the literature in cases of acute and chronic cholecystitis [10]. However, PET-CT is not a valuable tool to differentiate benign inflammation from malignancy; surgical excision and pathologic examination may be warranted to determine the exact underlying pathology. FDG PET-CT is not specific for differentiating cancer from cholecystitis; inflammation also reveal overexpression of GLUT1 and GLUT three leading to increased FDG avidity; however, FDG PET-CT seems powerful for diagnosing gallbladder pathology as a false-positive cause of CEA rising [9].
CONCLUSION
Elevated levels of carcinoembryonic antigen in the context of colon cancer surveillance, although likely suggesting residual/ recurrent disease, are not an specific test. Gallbladder and biliary system disorders should always be considered.
The case emphasizes that in context on negative imaging and still suspicious elevated CEA levels, particular attention to the biliary tree is beneficial.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}