





Abstract
Hereditary angioedema is a rare genetic condition causing episodes of angioedema—including life-threatening laryngeal oedema. Episodes can be unpredictable, or triggered by factors such as trauma, drugs or dental treatment. When faced with a patient with a fractured mandible, who has had a severe attack of angioedema when prescribed either ibuprofen or codeine based analgesia, this required an alternative approach to analgesia. Using a catheter and local anaesthesia, we were able to keep the patient comfortable, and pain free.
INTRODUCTION
Hereditary angioedema is caused by a deficiency or malfunction of the protein C1 inhibitor (C1-INH)—also called C1 esterase inhibitor. C1-INH is part of the complement system, coagulation system and fibrinolytic system.
Symptoms include [1]:-
Localised subcutaneous swelling:
o The oedema is circumscribed and non-pitting.
o There is no urticaria or itching.
o There may be prodromal burning, tingling, erythema or a serpiginous rash (erythema marginatum).
Abdominal symptoms:
o May give a clinical picture of intestinal obstruction or an acute abdomen with tenderness and guarding.
o Symptoms include abdominal pain (can be severe or sudden in onset), nausea and vomiting, diarrhoea, constipation and abdominal distention.
o Large fluid shifts with ascites or hypovolaemic shock may occur.
Treatment and management is with preventative medication such as Danazol, and acute flares are treated with C1-INH.
CASE REPORT
A 24-year-old male presented with an isolated fracture of the left angle of the mandible after an alleged assault. He reported that previously both Ibuprofen and Codeine based analgesia had led to severe exacerbations of Hereditary Angioedema, each requiring intubation and ventilation to prevent loss of the airway.
He was initially prescribed Paracetamol, which was unable to control his level of pain. The patient was listed for an open reduction and internal fixation of the mandible. There was a delay to theatre for the patient, while another patient had a prolonged procedure with a life-threatening emergency.
We decide to use a catheter for analgesia delivery to the Inferior Alveolar Nerve, as this could remain in situ for the whole perioperative period, and prevent the patient having repeated injections. The patient was much more comfortable and found the method of analgesia acceptable.
There was no exacerbation of his hereditary angioedema, and his course of treatment was unremarkable after he was covered by both Danazol and C1-INH under the guidance of his regular physician.
TECHNIQUE
The technique has been developed using single use items one would typically find in an accident and emergency or ward setting.
Figure 1 demonstrates a pre-operative set of items required for placement- disposable needle and syringe, local anaesthetic, 22 Gauge spinal needle, 3–0 silk suture, needle holders and suture scissors.
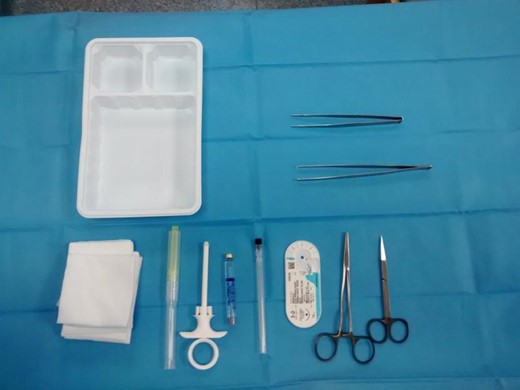
Equipment required for procedure.
Local anaesthetic is applied to the buccal mucosa to enable sutures to be placed to secure the cannula.
The catheter is placed in the same manner as an ID block, between the coronoid notch and the pterygomandibular raphe.
The needle is removed post insertion and disposed of correctly, and the catheter remains in situ.
DISCUSSION
Inferior alveolar blocks can be used for pain relief with mandibular fractures [2]. It helps to negate the need for the use of opioid based medication. This technique uses a spinal needle as a catheter. The catheter is inserted to enable the repeated delivery of long acting local anaesthetic such as bupivicaine to the Inferior dental nerve. The catheter, allows re-administration of analgesia in a quick, effective and non-invasive manner.
Patients awaiting definitive treatment for a fractured mandible often requires a prolonged period of being nil by mouth. This is because trauma occurs most frequently on the weekends [3], and this is when there is the most limited availability of theatre services [4]. The use of ID blocks and regional anaesthesia are well known to produce effective relief for mandibular fractures but do require a suitably trained person to deliver them, and repeated injection is not well tolerated by patients [5].
In addition the above factors many of the patients who suffer mandibular fractures tend to be under the influence of drink and/or drugs. This often means that producing a safe and clear medical and drug history can be difficult. Combined with this the risk of interactions of opioids with alcohol or illicit drugs [6], this technique allows safe and effective delivery of analgesia to the patient (Fig. 2).

Picture showing two sutures are placed to secure the catheter intra orally. The cannula is reviewed to ensure is doesn’t come into contact with the dentition.
To the best of the authors knowledge there have no reported cases of an intra-oral approach to produce pre or post-operative analgesia. The method could also be used with adapted techniques for patients with trismus. It also prevents the need for an extra-oral approach which may cause scarring and skin infection. The use of bupivicaine is well documented as an excellent method for long term analgesia, and does not have to be administered by a doctor/dentist once the catheter is in situ (Fig. 3).
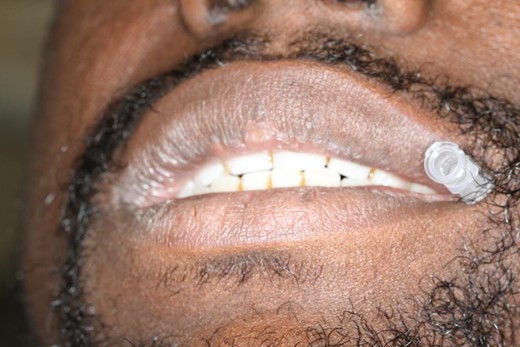
Picture showing the catheter portal accessibility for regular delivery of plain bupivacaine.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}