





Abstract
Hepatic artery avulsion following politrauma is an extremely rare condition with a very high mortality rate. Management is based on damage control surgery given the precarious situation of these patients. Ligating the artery is one option under such circumstances, despite potential consequences including ischemic cholangiopathy (IC). Ischemic cholangiopathy, which can be caused by an insufficient blood supply to the bile duct, generally results in stricture and recurrent cholangitis, and the need for a liver transplant in extreme cases.
We present the case of a 37-year-old male with multiple traumas after falling from the third floor of a building. He was hemodynamically unstable upon arrival at the emergencies department, with no improvement on administration of aggressive fluid therapy. A Echo-FAST exam evidenced fluid in all quadrants, so the patient was transferred to the operating room where a 4-litre hemoperitoneum secondary to total avulsion of the proper hepatic artery was observed. The patient required massive transfusion and vasoactive drugs, with instability throughout the intervention; therefore, we decided to ligate the proper hepatic artery. Hepatic dysfunction and diffuse IC with multiple episodes of recurrent cholangitis were observed during the postoperative period. Given the irreversible clinical picture, we opted for a liver transplant 70 days after the patient’s initial admission. The patient died on Day 34 post-transplant due to irreversible ischemic brain damage and a right occipital hemorrhage.
Hepatic artery avulsion due to trauma is very rare and its management very complex, and in certain situations the artery must be ligated. The main consequence of ligating the hepatic artery is IC, which is more frequently observed secondary to iatrogenic lesions or systemic diseases, while very few cases have been published in which IC is secondary to hepatic artery avulsion caused by hepatic trauma. Treatment depends on the extent of ischemia, and when the damage is diffuse, as in our case, it may involve a liver transplant.
BACKGROUND
The liver is the second most commonly injured organ following blunt abdominal trauma [1]. Injuries tend to be grade I–III [1], so they can be managed through nonsurgical treatment involving intensive care or interventional radiology, while the patient remains hemodynamically stable. Current mortality rates for hepatic trauma are around 0–8% depending on the grade of the injury [2]. Grade V–VI injuries are associated with hepatic avulsion or porta hepatis injury (grade III, Niamieno et al.). [3] It suppose such a challenge for any surgeon that, in extreme cases, liver transplantation may be the best therapeutic option [4].
CASE PRESENTATION
Here we present the case of a 37-year-old male with a psychiatric history and harmful use of alcohol and cocaine. He was admitted to emergency services after falling from the third floor of a building. The patient was hemodynamically unstable upon arrival and did not improve with aggressive fluid therapy. X-rays were taken of the pelvis and thorax, and a chest tube inserted in the left thorax due to pleural effusion with serosanguineous fluid discharge. A Echo-FAST was performed where abundant free fluid was observed in all the quadrants, being transferred to the operating room for an emergency laparotomy, evidencing a 4-liter hemoperitoneum secondary to an active arterial bleeding from a complete avulsion of the hepatic artery itself as well as multiple hepatic lacerations. The patient remained unstable throughout surgery, requiring massive transfusion and vasoactive agents, thus we decided to ligate the proper hepatic artery and perform temporary abdominal closure using the vacuum pack technique [5].
He was admitted to the Resuscitation Unit and after hemodynamic recovery, a CT scan was performed with no neurological lesions, confirming the findings observed intraoperatively as well as the absence of blood flow in the hepatic artery (Fig. 1).
Hepatic dysfunction (ALT 3 800, TBil 6, 74 000 platelets/μl, IP 40%), probably secondary to ischemic hepatitis, was observed during the immediate postoperative period. The abdomen was closed definitively three days after the trauma.

TAC reconstruction of hepatic artery avulsion.
On the seventh postoperative day (POD), discharge of bile contents was observed by the abdominal drainages. Therefore, given the suspicion of ischemic cholangiopathy (IC) and the poor clinical situation of the patient, a transparietohepatic cholangiography was performed for diagnostic and therapeutic intention, demonstrating a destructuring of the intra- and extrahepatic bile duct compatible with ischemic cholangiopathy, so an internal–external transhepatic drainage was inserted. After clinical improvement, the study was completed with an MRI that showed signs of multiple hepatic infarctions and diffuse IC (Fig. 2).
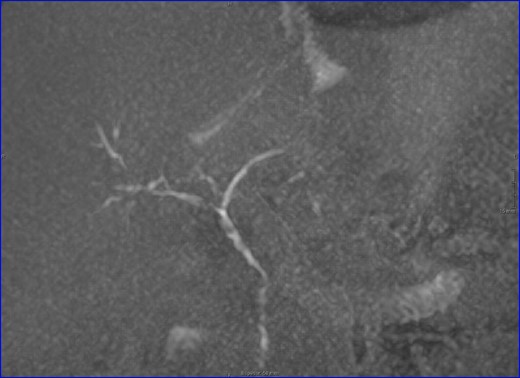
MRI: biliary tract, multiple stenosis. ischemic cholangiopathy.
After a slight clinical improvement, on POD 40, the patient developed a septic shock secondary to cholangitis with multiple bilomas observed on a CT scan.
Considering the irreversible IC, and after sepsis control, it was decided, in a multidisciplinary committee, to include it in the waiting list for liver transplantation [6]. The transplant was performed 70 days after admission, requiring biliary reconstruction with a hepaticojejunostomy
After the transplant, the patient required three re-operations and two arteriographies due to hemoperitoneum, without revealing the origin of the bleeding.
On day POD after the transplant, he presented bilateral mydriasis and decreased level of consciousness. The brain CT scan showed multiple bilateral ischemic lesions and a right occipital hemorrhage. After consulting with neurosurgery and in a multidisciplinary session, it was decided to limit the therapeutic effort, dying on POD 36 after transplantation.
DISCUSSION
Most of the hepatic traumas are mild, allowing a non-operative management. However, the literature contains very few cases of hepatic trauma with avulsion of the hepatic artery, which mortality rate is in the range of 50–100% [7]. The management of this clinical situation is very complex and determined by the patient’s hemodynamic status. Although attempts can be made to reconstruct the hepatic artery, the patient is generally in a precarious situation and the surgeon probably lacks experience of this scenario, so the most recommendable option could be damage control surgery, which usually involves ligating the hepatic artery and hepatic packing depending on the associated hepatic lesion [8].
The main consequence of ligating the hepatic artery is typically IC, as occurred in the present case.
Ischemic cholangiopathy is focal or diffuse damage to the bile duct secondary to an inadequate arterial blood supply. IC occurs because the hepatic artery is the only arterial supply to the bile duct, with 50% of the artery’s blood flowing to the bile duct.
The most common cause is artery stenosis or thrombosis after a liver transplantation [9], but IC could be secondary to any injury of the hepatic artery, namely in the case of arterial infusion of toxic agents such as intra-arterial chemotherapy, arterial embolization, advanced AIDS, radiotherapy, polyarteritis nodosa, or hemorrhagic telangiectasia syndrome.
Damage to the biliary tree causes necrosis, bile leakage, bilomas, fibrosis and stricture, which manifests clinically as recurrent cholangitis.
A diagnosis of IC should always be suspected whenever there are bile duct abnormalities in the context of an intervention or a systemic process that could affect arterial flow.
The diagnosis of suspicion is confirmed with laboratory tests, wherein we can detect a cholestatic pattern through elevated levels of alkaline phosphatase, gamma-glutamyl transferase and bilirubin, which could give rise to liver failure in more advanced cases. The clinical picture is based around recurrent cholangitis. An MRI is the test of choice to confirm this suspicion, which in the first stage manifests with biliary casts or bilomas, whereas multiple, irregular strictures appear in advanced stages.
Treatment should be individualized depending on the patient’s signs and symptoms and the extent of their injuries. Focal damage can be managed conservatively through dilatation and endoscopic or percutaneous drainage and stent placement. However, in the case of diffuse injury, transplant could be the treatment of choice once the septic process is under control [10].
CONCLUSIONS
Liver trauma is a very uncommon cause of liver transplantation. Nevertheless, hepatic artery injuries due to trauma lesion may need arterial ligation leading to the development of ischemic cholangiopathy. Liver transplantation may be indicated in cases of severe ischemic cholangiopathy
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}