





Abstract
Diaphragmatic hernia in the absence of trauma in adults is very rare. It occurs as a result of unilateral diaphragmatic agenesis. The diagnosis of this rare condition is typically made in early infancy. However, in asymptomatic patients, the diagnosis is often delayed for months and even years. We present a case of a 27-year-old female, who was referred 48-hours after Caesarean section with suspected pulmonary embolism. Computed tomography scan revealed herniation of the liver as well as bowel loops into the right hemi-thorax. Exploration through a right thoracotomy revealed right diaphragmatic agenesis. The contents were reduced into the abdomen, and the defect was repaired using a mesh. The patient had an uneventful postoperative recovery and was discharged home 10 days later. This case highlights the acute late presentation of right diaphragmatic eventration with abdominal visceral herniation in adulthood. The condition may be triggered by the increasing size of gravid uterus.
INTRODUCTION
Diaphragmatic hernias can be either congenital or acquired. The congenital variety occurs in 0.45 cases per 1000 births due to failure of the muscular entities of the diaphragm to develop normally, resulting in displacement of abdominal components into the thorax [1]. In most patients, it presents early in life but smaller congenital hernias may go undetected during childhood and present later in adult life [1]. In adults, right-sided diaphragmatic hernias are less common than those in the left side, and are usually of the acquired type, caused commonly by penetrating or blunt trauma [2]. This type of herniation typically presents with strangulation requiring rapid diagnosis and necessitating urgent surgical intervention [3].
We report a case of a right-sided congenital diaphragmatic hernia in an adult female presenting with respiratory distress which was misdiagnosed as pulmonary embolism 2 days after an elective Caesarean section.
CASE REPORT
A 27-year-old female patient was referred from another facility with the suspicion of pulmonary embolism 48-hours post elective Caesarean section. She denied any history of chest pain or haemoptysis. She also denied any recent or past history of chest trauma and was not known to have any past medical illnesses.

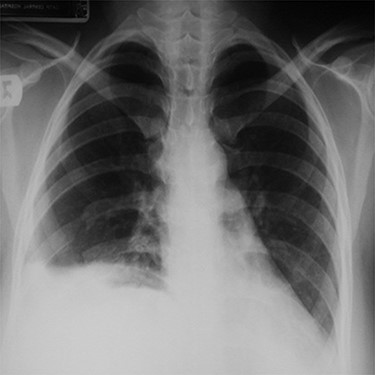
Chest x-ray (on arrival) showing a homogeneous opacity (the liver) occupying the right hemi-thorax with some bowel loops the right hemi-thorax with obvious mediastinal shift to the left side.
Upon arrival, she was in respiratory distress with tachypnea (RR: 25/min) and tachycardia (116/min), but normal blood pressure (130/80). Chest examination revealed diminished air entry and dull percussion on the right side. Abdominal examination was unremarkable.
Her routine laboratory investigations including white cell count were normal. Electrocardiogram showed sinus tachycardia. Chest x-ray showed homogeneous opacity occupying the right hemi-thorax, and bowel loops were seen above the right chest with obvious mediastinal shift to the left side (Fig. 1). Abdominal computed tomography (CT) scan with contrast
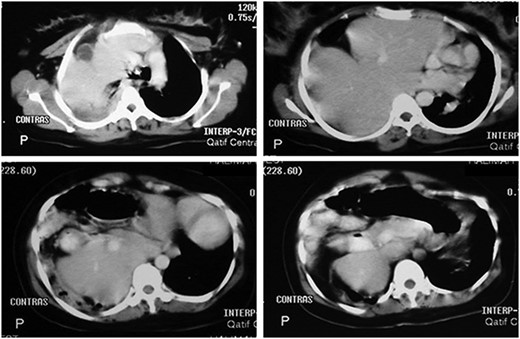
Abdominal CT scan with contrast showing the entire liver and some bowel loops occupying the right hemi-thorax.
showed the entire liver and some bowel loops in the right hemi-thorax (Fig. 2). The impression was right diaphragmatic herniation, although ruptured right hemidiaphragm was entertained despite the negative history of chest trauma.
The patient was prepared for surgery. The chest was opened through a right posterolateral thoracotomy. The right hemi-diaphragm was found to be absent and the liver was lying high up in the right thorax with its inferior surface adherently facing the pericardium. The right lung was collapsed, and the transverse colon and the stomach were also found in the right hemi-thorax inferiorly. The liver was carefully mobilized from the pericardium and the herniated organs were successfully reduced into the abdomen. After excision of the thin hernia sac, the right diaphragm was reconstructed using a polypropylene mesh. The right lung expanded well at the end of the procedure. Postoperative chest x-ray showed full inflation of the right lung (Fig. 3).
A post-operative chest x-ray showing full inflation of the right lung.
The postoperative recovery was uneventful and the intra-abdominal pressure remained within the normal range during monitoring for 24 hours. The patient was discharged on the tenth postoperative day and remained well with no evidence of recurrence at 18-month follow-up.
DISCUSSION
The first reported case of diaphragmatic agenesis in adult was described in 1988 by Tzelepis et al. in a patient presented with a persistent left lower lobe infiltrate that was ultimately determined to be complete absence of the left hemi-diaphragm [4]. The condition is rare, resulting in congenital diaphragmatic herniation in approximately one in 4000 live births [5]. The diagnosis is typically made very early in infancy and carries a significant mortality of up to 38–62% [2, 5, 6]. Survival often depends on cardiopulmonary function and the presence or absence of other congenital anomalies [5]. Smaller hernias which commonly arise in the posterolateral congenital diaphragmatic defects are usually asymptomatic and may remain undiagnosed until adulthood [3, 5].
Agenesis of the hemi-diaphragm is left-sided in 88–97% of cases, and right-sided defects are less common because of the earlier closure of the right pleuroperitoneal hiatus [5, 7]. Moreover, the liver tends to prevent herniation through any diaphragmatic defect that might be present on the right side [3]. Various studies have reported left-sided diaphragmatic hernias containing colon, stomach, momentum, spleen, small bowel, pancreas and adrenal gland, whereas the documented contents of right-sided hernias have been limited to liver, gallbladder, kidney and omentum [5].
The herniation may remain asymptomatic but in some cases, the first manifestation appears as a result of increased intra-abdominal pressure, such as that occurring during pregnancy [3, 5]. Progressive herniation may cause bowel obstruction and subsequent infarction [4]. Late presentation of the right hemi-diaphragm agenesis with visceral herniation into the thoracic cavity—as in this case—is very rare to find in an adult who has suffered no blunt or penetrating trauma to the lower chest [2]. Our patient had no symptoms prior to her pregnancy as the liver was apparently still within the abdominal cavity until it was probably displaced into the thorax by the enlarging of the gravid uterus. Also, there was no evidence of respiratory events during the Cesarean section.
Adult patients with right-sided agenesis require operative intervention to prevent liver as well as other abdominal organ herniation [7, 8]. Operative intervention is also required in symptomatic patients with dyspnea or organ herniation to prevent worsening of pulmonary function or organ damage [6–8]. The hernia can be dealt with through either thoracic or abdominal approach. Combined thoraco-abdominal approach can be adopted in difficult cases and it provides good surgical exposure and easy access to the abdomen, if needed [4]. Minimally invasive technique can also be adopted to repair the hernia [9]. We adopted a thoracic approach which served the purpose of reducing the contents, excising the thin hernia sac and repair the defect very well. After restoring the herniated organs into the abdominal cavity, diaphragmatic reconstruction can be performed using a tension-free polypropylene or expanded polytetrafluoroethylene mesh [6, 10].
In this case, it was interesting to see the immediate expansion of left lung after alleviating the pressure effect of the herniating abdominal organ. This indicates that there was no associated ipsilateral lung agenesis and that the herniation of abdominal viscera happened recently as a result of the increasing size of the gravid uterus leading to the sudden post-operative symptoms of dyspnea and tachypnea which mimicked pulmonary embolism and prompted referral to our facility.
CONCLUSION
Unilateral right-sided hemi-diaphragm agenesis is an exceedingly rare diagnosis in adults. It may present acutely with sudden onset of respiratory distress; mimicking pulmonary embolism. The definitive diagnosis requires a high index of clinical suspicion as routine imaging studies may miss subtle evidence of diaphragmatic defects. Repair of right-sided defects is necessary in symptomatic patients to prevent decline in pulmonary function and prevent visceral herniation. In child-bearing women, repair of the defect may be warranted even if asymptomatic to prevent visceral herniation during pregnancy.

{kind=link}
{kind=link}
{kind=link}