





Abstract
Intussusception is a rare cause of bowel obstruction in adults, and has generally an organic etiology. However, adenomatous polyp of the small bowel is an uncommon etiology. Moreover, there’s a great difference with childhood intussusception in its presentation, etiology and management. We describe herein a case of adult ileocecal intussusception due to an adenomatous ileal polyp with a preoperative diagnosis made on computed tomography. We performed a right hemicolectomy, without attempting to reduce the intussusception, and an end-to-end ileotransverse anastomosis. The pathological examination of the surgical specimen revealed an adenomatous polyp with a high grade dysplasia on the terminal ileum, being the cause of the ileocecal intussusception.
INTRODUCTION
Adult intussusception is a rare condition which accounts for 1% of patients having bowel obstruction, and 5–10% of all intussusceptions cases [1]. The preoperative diagnosis is difficult, given the variability of presentations. The etiologies are numerous and among these, adenomatous polyp of the small intestine is very uncommon. We report a case of adult intussusception due to an adenomatous polyp of the small intestine which was diagnosed preoperatively by CT scan. We aim to discuss the diagnosis and therapeutic modalities of this entity.
CASE REPORT
A 50-year-old Senegalese male presented to the emergency unit, with acute abdominal pain initially localized in the right lower quadrant, then generalized to the whole abdomen, lasting for 5 days. The pain was associated with vomiting related to food intake, and alteration of bowel habits. There was neither fever, nor relieving factors and he had a non-contributory past medical history, apart from a recent minimal weight loss.
Physical examination revealed a minimal dehydration with an abdominal distension. The rectal examination was normal. The vital signs including the temperature, the pulse, the blood pressure and the respiratory frequency, were within normal limits.
A plain abdominal radiography suggested a bowel obstruction, by showing multiple air-fluid levels. Biological results were the following: hemoglobin: 13,5 g dl−1, hematocrit rate: 42,5%, white blood cell count: 8×103 mm−3, creatinine = 18 mg L−1, serum Na: 139 m Eq L−1, serum K: 3.4 m Eq L−1. The contrast-enhanced CT showed a target mass localized in the right iliac fossa, and was suggestive of ileocecal intussusception without specifying the underlying cause (Fig. 1). While coronal reconstruction showed a « sausage-shaped mass » (Fig. 2). Moreover, there was some lymphadenopathies surrounding the target mass, and a small amount of abdominal effusion.
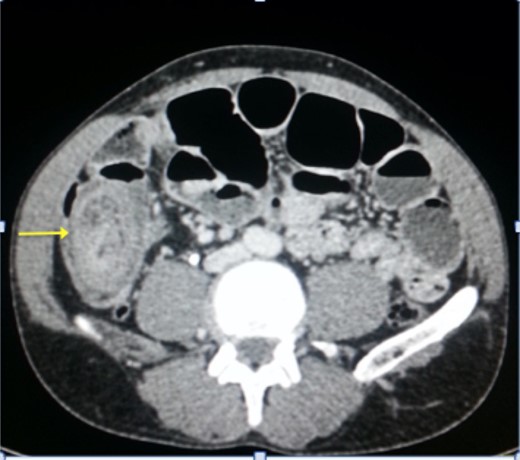
Axial section of abdominal CT showing the‘target mass’.

Coronal reconstruction of abdominal CT showing the ‘sausage sign’ of ileocecal intussusception.
Upon laparotomy, we found an ileocecal intussusception, with mesenteric lymphadenopathies and a dilation of the whole small bowel (Fig. 3). We performed a right hemicolectomy, without attempting to reduce the intussusception, and an end-to-end ileotransverse anastomosis.
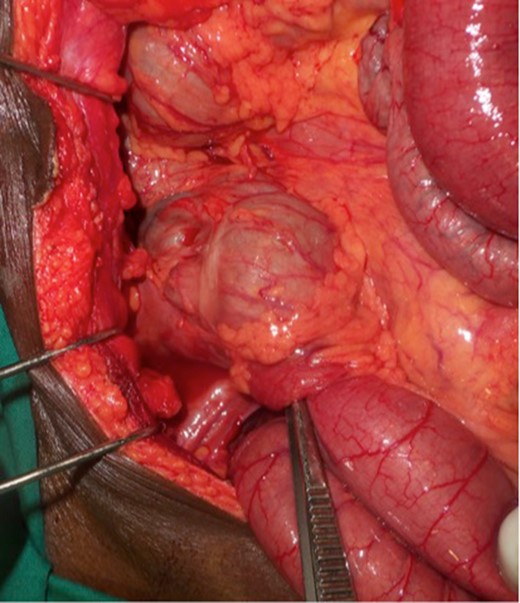
Intraoperative view of the ileocecal intussusception.
The post-operative outcomes were favorable. The pathological examination of the surgical specimen found an adenomatous ileal polyp with a high grade dysplasia on the terminal ileum being the cause of the ileocecal intussusception (Fig. 4).
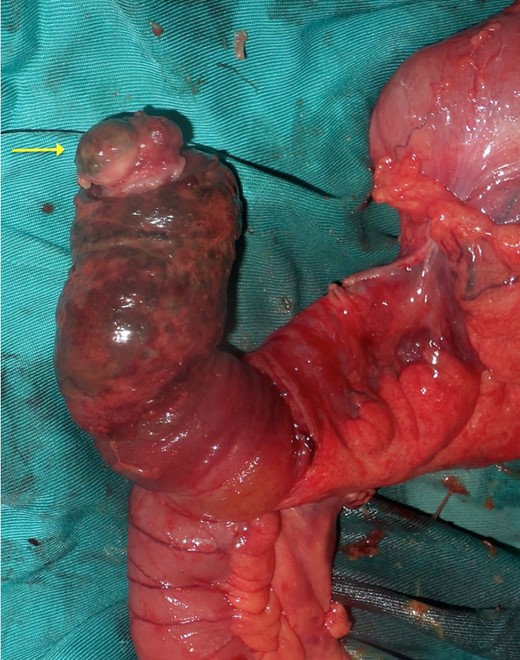
View of the surgical specimen with the ileal polyp.
DISCUSSION
Intussusception in adults is rare, although being frequent in children [1].
There is a great difference with childhood intussusception in its presentation, etiology and management [1–3]. In adults, acute presentation is reported to be rare in contrary with children [3, 4]. Indeed, several studies found chronic non-specific symptoms being the most frequent presentation in adults [3–5]. Our patient presented symptoms of acute bowel obstruction. The diagnosis is often delayed in adults given the unspecific presentation and rarity [3]. The commonest symptoms are nausea or vomiting, abdominal colic, change in bowel habits, rectal bleeding and a palpable mass. The classical triad of cramping abdominal pain, abdominal mass and bloody diarrhea is rarely found in adult and was not present in our patient [3, 4].
Computed tomography (CT) scan is the most sensitive imaging modality for the diagnosis of intussusception with a diagnostic accuracy ranging from 58 to 100% [2, 3, 6, 7].
The classic ‘target mass’ picture on CT scan as found in our case, is pathognomonic of intussusception [6]. It consists in a central dense area and a halo of low attenuation being respectively the intussusceptum and the edematous intussuscepiens [7, 8]. In a sagittal view, we found the classical « sausage sign » in our patient. Moreover, CT scan may identify the underlying cause of the intussusception [1]. The common sites of occurrence of this condition are the junction between the movable segments of the intestine and segments that are relatively fixed as in our case.
Almost 90% of adults with intussusception have an underlying lesion, nearly half of which are malignant [3, 6, 9]. While in pediatric population, a predisposing cause is rarely found [3, 10]. Therefore, unlike children, reduction is not a therapeutic modality in adults given the high risk of underlying malign lesion [2, 3].
However, controversy remains about the management of adult intussusception [3]. Indeed, according to some authors, a gentle reduction is possible before performing the resection in case of high suspicion of benign lesion for small bowel intussusceptions.
This conservative strategy is more relevant in situations requiring resection of a long portion of bowel as well as in patients with post-operative bowel obstruction, providing an absence of ischemia or strangulation.
However when the large bowel is involved, surgical resection is recommended due to the high risk of underlying malignancy, perforation and spillage [2, 8].
In our patient, we did not attempt to reduce the intussusceptum because of the probability of a malignant lesion given the lymphadenopathies and the large bowel that was involved. Laparoscopic management has been reported to be a safe and feasible option regardless of the etiology [3].
CONCLUSION
Adult intussusception is a rare entity. Given high risk of malignancy, reduction is most often prohibited and surgical resection either via laparoscopy or laparotomy is the best therapeutic attitude.
ACKNOWLEDGEMENTS
None.
CONFLICT OF INTEREST STATEMENT
I confirm that none of the authors have any competing interests.
FUNDING
Not applicable.

{kind=link}
{kind=link}
{kind=link}
{kind=link}