





Abstract
We compare two surgical approaches for segmental tracheal resection for tracheal cancer: cervical collar incision with median sternotomy and right posterolateral incision. In case one, a 46-year-old woman presented with adenoid cystic carcinoma, measuring 4.5 cm longitudinally, located at the junction of the cervical and mediastinal trachea. Cervical collar incision with median sternotomy provided a good exposure of the entire trachea. Although a relatively long tracheal resection (5.0 cm) was required, sufficient mobilization of the entire trachea facilitated low-tension anastomosis. In case 2, a 39-year-old man presented with squamous cell carcinoma, measuring 1.8 cm longitudinally, located at the lower trachea 1.8 cm from the carina to the proximal side. Right posterolateral incision provided a good exposure of the lower trachea. Although the required tracheal resection was relatively short (3.0 cm), the anastomotic tension was high. The high anastomotic tension was likely attributed to the limited mobilization of the proximal trachea.
INTRODUCTION
Tracheal segmental resection is the treatment choice for primary tracheal cancers. Approaches for this surgical technique, e.g. cervical collar incision with median sternotomy and right posterolateral incision, are commonly chosen according to the tumor location. However, to date, adaptive criteria based on the reduction of the anastomotic tension that respective surgical approaches can facilitate in varying degrees have not been adequately discussed. Thus, ensuring low-tension anastomosis is one of the key points to avoid anastomotic complications. Here, we compare these two surgical approaches focusing on the tracheal mobilization available in each procedure for decreasing anastomotic tension.
CASE 1
A 46-year-old woman presented with wheezing. Chest computed tomography (CT) revealed a folding-fan-shaped mass in the tracheal lumen, measuring 4.5 cm longitudinally along the trachea, involving the right wall of the junction of the cervical and mediastinal trachea (Fig. 1a). Trans-bronchial biopsy (TBB) of the mass demonstrated adenoid cystic carcinoma (ACC). Radiological workups for locoregional lymph node or distant metastasis were negative (cT4N0M0). Because the tumor was located in the upper part of the trachea, and the estimated tracheal length for segmental resection was relatively long (>4.5 cm), the surgery was initiated with cervical collar incision and median sternotomy for fully mobilizing the overall length of the trachea to reduce anastomotic tension. Therefore, the superior vena cava and ascending aorta were mobilized followed by exposure of the entire trachea by incising the posterior pericardium and mobilizing the right pulmonary artery. We could easily mobilize the anterior and bilateral walls of the trachea from the cervical level to the left and right main bronchi origins (Fig. 1b). Proximal and distal margins for segmental tracheal resection were intraoperatively determined via observation of grossly normal airway using flexible bronchoscopy. Tracheal segmental resection was simultaneously accomplished via the establishment of a cross-field ventilation. The resected specimen measured 5.0 cm (8 tracheal cartilage rings) longitudinally (Fig. 1c). Although both proximal and distal margins tested positive from frozen sections, additional tracheal resection was not performed to ensure low-tension anastomosis. The membranous and cartilaginous tracheae were anastomosed using a running 4-0 polydioxanone (PDSII, Ethicon, Somerville, NJ) and interrupted 3-0 polydioxanone sutures, respectively, at a low degree of tension. Adjuvant radiotherapy (60 Gy) was started at two months after the surgery, after which bronchoscopy confirmed satisfactory epithelization of the anastomotic part.
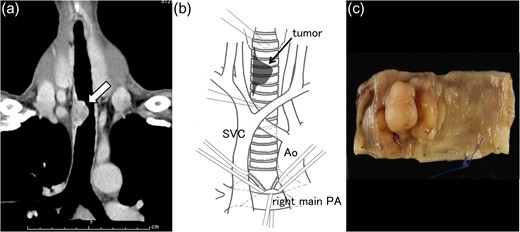
Chest computed tomography revealed a mass (arrow), measuring 4.5 cm along the longitudinal axis of the trachea, involving the right wall of the junction of the cervical and mediastinal tracheae (a). Cervical collar incision with median sternotomy provided sufficient mobilization of the entire trachea; from the cervical level to the left and right main bronchi origins (b). The resected specimen measured 5.0 cm (eight tracheal cartilage rings) longitudinally (c).
CASE 2
A 39-year-old man presented with a cough, dyspnea and hemosputum. Chest CT revealed a 1.8 cm mass located in the tracheal lumen that involved the right wall of the lower trachea (Fig. 2a). TBB of the mass demonstrated squamous cell carcinoma (SqCC). All radiological workups for metastases tested negative (cT4N0M0). The tumor was located in the lower trachea (1.8 cm from the carina to proximal side); therefore, the surgery was initiated with a right posterolateral incision. After thoracotomy, the trachea was exposed from the level of the brachiocephalic artery to the right main bronchus (Fig. 2b). Tracheal segmental resection was accomplished using the same procedure as described in case 1. The resected specimen measured 3.0 cm (six tracheal cartilage rings) longitudinally (Fig. 2c), and both sides of margins were negative for malignancy, as confirmed by microscopic analysis. To ensure low-tension anastomosis, we utilized the following additional release maneuvers: sufficient cervical flexion; division of the right pulmonary ligament; and incision of the pericardium around the right hilum. Anastomotic procedures were also same as those used in case 1. Although the length of the resected trachea was shorter than that in case 1, the anastomotic tension was relatively high such that further sufficient circumflex dissection of the proximal trachea was required to gain anastomotic approximation with an acceptable degree of tension. Follow-up bronchoscopy demonstrated a well-epithelized anastomotic part.
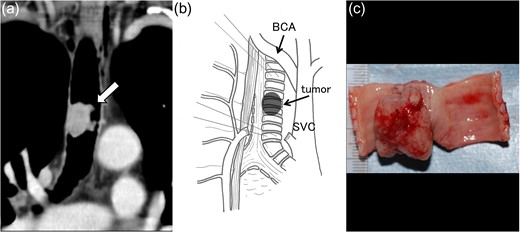
Computed tomography revealed a mass (arrow), measuring 1.8 cm longitudinally, involving the right wall of the lower trachea (a). Right posterolateral incision provided sufficient exposure of the lower trachea (b). The resected specimen measured 3.0 cm (six tracheal cartilage rings) longitudinally (c). Ao, Aorta; SVC, superior vena cava; PA, pulmonary artery; BCA, brachiocephalic artery.
DISCUSSION
There is limited literature that describes surgical approaches for segmental tracheal resection depending on tumor locations. Grillo and Mathisen [1] derived an adaptive criterion of approaches for tracheal tumors: upper tracheal tumors were exposed by cervical collar incision, midtracheal tumors cervical collar incision were extended to full median sternotomy, and lower tracheal tumors were most often approached through a right thoracotomy. Keshavjee and Pearson [2] utilized right thoracotomy for tumors located at the distal one-third of the trachea and employed a cervical collar incision with an option of median sternotomy for tumors located at other regions of the trachea.
Literature discussing surgical approaches according to the length of the trachea needed for resection is scarce, but there is regular consensus regarding limits of tracheal resection. Mulliken and Grillo [3] demonstrated that approximately half of the trachea could be excised and reconstructed with primary anastomosis by utilizing several release maneuvers for reducing anastomotic tension. However, Wright et al. [4] demonstrated that resections >4 cm were associated with a drastic increase in anastomotic complications. Longer resections tend to result in more frequent anastomotic complications, which are attributed to tracheal devascularization and excessive anastomotic tension.
In our initial case, requiring a relatively long resection of the trachea which exceeded the safety limit, cervical collar incision with median sternotomy provided sufficient exposure for mobilizing the entire trachea to reduce anastomotic tension. This approach will provide considerable advantages in cases requiring a longer resection of the trachea than preoperatively estimated, particularly in ACCs that have a proclivity of extending for long distances submucosally [1].
Our second case demonstrated that right posterolateral incision provided adequate exposure of the lower carina. Although the length of the resected trachea in this case was shorter than that resected in case 1, the anastomotic tension in this case was relatively high, irrespective of the adopted maximal release maneuvers as reported by Liberman and Mathisen [5]. We surmise that because there are considerable individual differences in the extent of exposable trachea in upper mediastinum during right thoracotomy, the relatively high anastomotic tension in the second case may be attributed to the limit of proximal trachea dissection. In case of lower tracheal tumors, which are anticipated to require relatively long resection of the trachea, median sternotomy with broad tracheal mobilization could be considered as an alternative to ensure safe anastomosis.
CONFLICT OF INTEREST STATEMENT
I declare on behalf of my co-authors and myself that we do not have any conflict of interest to declare.

{kind=link}
{kind=link}