





Abstract
A 69-year-old woman was admitted electively for a laparoscopic cholecystectomy. Pre-operatively she had an ultrasound abdomen which demonstrated a large gallbladder (GB) stone. Intraoperatively, a nodule was noted on the liver supero-lateral to GB. The procedure was subsequently converted to open and the lesion was resected en-bloc with GB. The histology result showed small cell carcinoma (SCC) of the gallbladder with invasion into the liver parenchyma. A staging computerized tomographic of the thorax, abdomen and pelvis was performed. This demonstrated enlarged adenopathy locally and systemically with metastasis to medial segment of the left hepatic lobe and right lung. Following multi-disciplinary team meeting she was referred to Oncology for chemotherapy. The patient has survived for 7 months after the initial diagnosis of SCC.
INTRODUCTION
Gallbladder cancer (GBC) is a rare malignancy and has a poor prognosis [1]. Interestingly, most GBC cases are diagnosed incidentally in cholecystectomy specimens. Gallstones are present in ~90% of GBC [2]. GBC tends to be more common in elderly women [3]. Other risk factors include gallbladder polyps, particularly adenomatous polyps, chronic infection with Salmonella typhi, congenital biliary cysts and genetic predisposition [4].
Small cell carcinoma (SCC) was first described by Albores-Saavedra in 1981 [5]. It is extremely rare tumour as only 72 cases were reported in the literature between 1981 and 2015, most cases were in Mexico, Japan, the USA and only one case in the UK [5]. To best of our knowledge, this is the first case reported in the Republic of Ireland.
CASE REPORT
A 69-year-old woman, presented to emergency department with intermittent upper abdominal pain for 1 year. The pain was most intense in the previous 2 days, she described it as gnawing pain, radiating to the right shoulder and associated with nausea. She denied any bowel or urinary symptoms. She was on Eltroxin 150 µg for hypothyroidism and she was an ex-smoker.
On examination, her abdomen was soft with moderate epigastric tenderness, Murphy’s sign was negative, there was no guarding or rigidity and bowel sounds were audible.
Her investigation showed a white cell count of 8 × 109/L, haemoglobin of 12 g/dL, bilirubin of 9 mmol/L, alkaline phosphatase of 84 IU/L, GGT of 17 IU/L, amylase of 46 U/L, C-reactive protein of 6 mg/dL. She had a previous ultrasound (US) abdomen in July 2014 demonstrating a single large gallstone (Fig. 1). The common bile duct (CBD) calibre was normal.
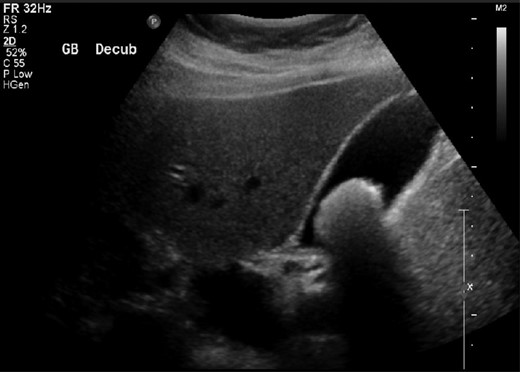
Abdominal US scan demonstrating a large gallbladder stone.
She was treated as biliary colic, discharged home and subsequently booked for an elective laparoscopic cholecystectomy.
The patient was admitted for an elective laparoscopic cholecystectomy a few months after. At laparoscopy, there were significant adhesions around Hartman’s pouch. There was also a suspicious nodule noted on the liver surface supero-lateral to GB. The decision was made to convert the operation to open. A retrograde cholecystectomy was performed with en-bloc resection of the lesion. The liver texture appeared normal and there was no enlarged regional lymph node identified, however, a single gallstone was noted. The patient recovered well and was discharged home on the fifth post-operative day.
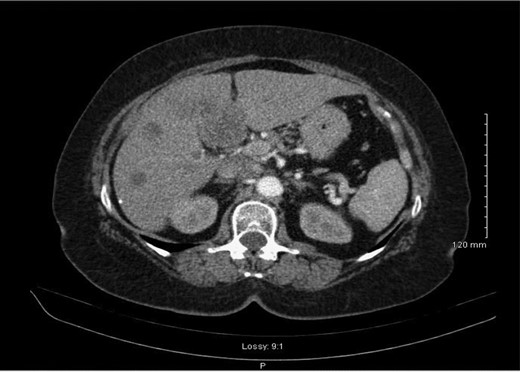
Histology demonstrated a 2.5 cm opaque stone and small cell undifferentiated carcinoma with tumour present in all layers of the gallbladder and lympho-vascular structures with invasion into the liver parenchyma. A subsequent staging computerized tomographic (CT) thorax, abdomen and pelvis demonstrated involvement of the lymph nodes within the coeliac axis and the porta hepatis, 3 mm nodular density in the right upper lobe of the lung and evidence of a metastatic deposit in the medial segment of the left hepatic lobe (Fig. 2). However, her completion staging CT brain revealed normal appearance.

Abdominal CT scan demonstrating metastasis to medial segment of left hepatic lobe.
Following review of the case at a multi-disciplinary meeting, the patient was referred to oncology. A consultation was also sought from hepatobiliary which indicates that she is extremely unlikely to benefit from any liver resection as the disease has progressed far to the lung and systemic lymph nodes, however, chemotherapy and a follow-up CT were suggested. She had three cycles of chemotherapy with Cisplatin and Etoposide, and a follow-up staging CT scan demonstrated progression of the disease, predominantly in the liver with new five lesions (Fig. 3), therefore, Cisplatin and Etoposide were stopped and she was switched to second line chemotherapy in form of FOLFIRI 20% dose reduction.
Re-staging abdominal CT scan demonstrating progression of the disease.
The disease progressed aggressively within the following few months, and she required admission to the hospital on a few occasions with repeat hyponatraemia as a para-neoplastic syndrome of her cancer. She continued to deteriorate and she died 7 months after the initial diagnosis of SCC.
DISCUSSION
SCC represents a highly aggressive rare tumour which is normally metastases upon presentation. Histologically, SCC consists of small round or oval atypical cells with scanty cytoplasm, hyperchromatic nuclei with cytoplasmic neurosecretory granules and inconspicuous nucleoli growing in sheets and cords [6]. Neuroendocrine cells normally are not seen in the GB mucosa [7]. However, they may develop in intestinal or gastric metaplasia of the GB mucosa and may also occur secondary to chronic cholecystitis and cholelithiasis.
Most of SCC cases present late because patients usually present with vague or non-specific symptoms which may be attributed to gallstones disease. Prognosis of SCC is poor with a median overall survival of 13 months mainly due to the late presentation of patients [8].
Treatment of SCC requires a multi-disciplinary approach involving surgery and oncology. The standard surgical treatment for SCC is cholecystectomy, and liver resection should be done if there is liver invasion [9]. Treatment with adjuvant chemotherapy did not show any improvement in overall survival of the regional disease, however, it did demonstrate a significant benefit in overall survival for SCC with distant metastasis compared to no chemotherapy [10]. Palliative radiotherapy in the form of prophylactic cranial irradiation and consolidation radiotherapy to the primary tumour bed and surrounding affected tissues liver may have a role in selected cases.
The case presented suggests that special consideration should be made in elderly women with a large single gallstone as this could be a risk factor for SCC, also it indicates that any suspicious lesion in the gallbladder’s bed should be biopsied when an elective cholecystectomy is being done. However, there was a limitation in this case in that there is no hepatobiliary service in our institution to help with the management of such cases.
CONCLUSION
Small cell carcinoma of the gallbladder is a very rare tumour with poor outcome. Early diagnosis, liver resection and chemotherapy are associated with a better survival. Further studies are required to identify patients at higher risk and improve outcome.
CONFLICT OF INTEREST STATEMENT
The authors have no areas of conflict to declare.
FUNDING
The authors have not received funding.
PATIENT CONSENT
The patient has passed away and relatives cannot be traced; all details have been sufficiently anonymized.
AUTHORS’ CONTRIBUTION
The case report was written by MA Zarog with input from EM Lyons and DP O’Leary and was edited by GJ Byrnes.

{kind=link}
{kind=link}
{kind=link}