





Abstract
Inverted papilloma of the urinary tract is a rare benign lesion. A 59-year-old male who presented with the chief complaint of gross hematuria and acute urinary retention is described. Cystoscopy revealed a solitary, papillary tumor at the bladder neck. Transurethral resection was performed, and histological examination revealed a pathological diagnosis of inverted papilloma. Following resection, the patient was able to void without difficulty. This is an interesting case of acute urinary retention secondary to an inverted papilloma at the bladder neck causing intermittent outlet obstruction, and we review the literature on inverted papilloma of the bladder.
CASE REPORT
A 59-year-old male was evaluated for gross hematuria and acute urinary retention requiring Foley catheterization in the emergency department. The patient did not have a family or personal history of urinary tract disease. He had no significant past medical history. He was a current smoker. Digital rectal exam revealed a 30 g symmetrical prostate with no nodules or indurations, and physical exam was otherwise unremarkable. Urinalysis was benign. Bladder ultrasound was suggestive of a polypoid bladder lesion arising at the bladder neck.
Cystoscopy showed normal anterior and posterior urethral segments with no strictures. The prostate was small with a somewhat tight bladder neck. There was a solidary 3-cm papillary lesion on a small stalk at the right of the bladder neck, reaching most of the way across the bladder to the left side.
The patient underwent transurethral resection of the bladder tumor, followed by cystolitholapaxy for several small bladder stones and transurethral resection of the prostate with bladder neck incision. Subsequently, the patient was able to void without difficulty.
Pathology demonstrates inverted urothelial proliferation with interconnected nests and trabeculae focally connected to overlying unremarkable benign reactive urothelium (Fig. 1). The lesion was well circumscribed. There was no exophytic papillary component, and the lesional cells were predominantly bland. There were some areas of mild atypia, with a degenerative appearance, but there was no mitotic activity or necrosis. Keratinizing squamous differentiation was not identified.
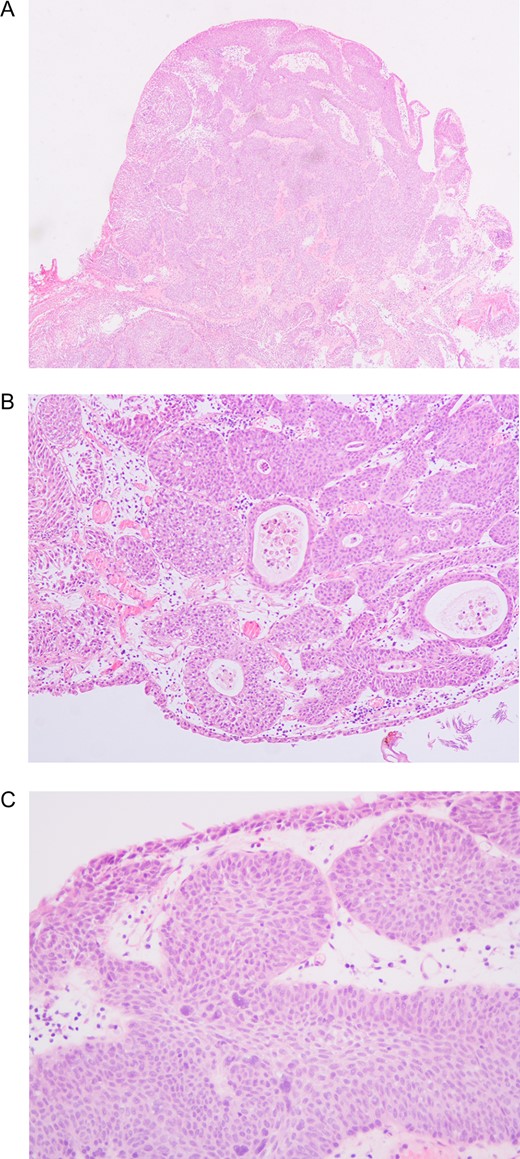
(A) Low magnification showing circumscribed inverted growth pattern with anastomosing nests and trabeculae of urothelial cells just beneath and connected to the smooth surface of benign urothelium (10×). (B) Medium magnification showing occasional microcysts in the inverted urothelial nests (25×). (C) High magnification showing occasional focus of mild epithelial atypia with a degenerative appearance of the nuclei (40×).
DISCUSSION
Inverted papilloma is rare benign tumor that can occur at any site in the urinary tract, but is primarily present in the bladder. Inverted papilloma of the bladder (IPB) accounts for 1.4–2.2% of all urothelial neoplasms [1]. The most commonly reported sites of IPB are at the bladder neck region (23–41%) and trigone (24–35%). Generally, the neoplasms are single lesions, though some cases may be multiple lesions (0–4.2%) [2]. Here, we described a solitary IPB located at the bladder neck.
IPB is most commonly diagnosed in the elderly, age 60–70, and is seen more often in men, with a ratio of 7.3:1 men to women. At present, the cause of IPB remains unclear, although it has been suggested that IPB is related to smoking, chronic bladder infection, and urinary tract obstruction [3]. In the present case, the patient’s current smoking status was an identifiable risk factor. It is however unclear whether low-grade obstruction due to a tight bladder neck predisposed the patient to developing IPB, or whether the location of the IPB at the bladder neck led to intermittent bladder outlet obstruction.
Clinically, patients with IPB have symptoms similar to patients with urothelial cell carcinoma, and often present with intermittent and painless macroscopic hematuria or dysuria due to urothelial irritation. In this case, in addition to gross hematuria, the patient presented with obstructive voiding symptoms likely secondary to the location of the IPB.
On MRI, the typical appearance of inverted papilloma of the bladder is a polypoid shape mass with a non-papillary surface and a thin short stalk surrounded by urine. Cystic foci are also occasionally seen within the tumor [4]. However, diagnosis requires direct visualization and biopsy.
On cystoscopy, IPB presents primarily as a pedunculated, such as papillary, polypoid and seaweed-like, or sessile mass with a smooth surface. IPB are typically 1–2 cm in size, but can sometimes be much larger, with diameter of up to 8 cm, and the current lesion is within the size range of IPB.
The diagnostic criteria for the pathological diagnosis of IPB are: (i) inverted growth pattern; (ii) smooth surface lined with mature urothelium; (iii) uniform epithelial morphology; (iv) tumor cells with consistent network of trabecular and smooth contour nested arrangement; (v) no or few mitotic figures; (vi) possible presence of microcyst formation; (vii) possible presence of non-keratinizing squamous metaplasia; (viii) no exophytic component; and (ix) noninvasive [5]. The current lesion was consistent with the diagnosis of IPB.
For management of IPB, transurethral resection of the bladder tumor is recommended as the standard of treatment. In addition, partial excision of the bladder may be necessary for relatively large neoplasms. IPB is considered a benign lesion, and incidence of tumor recurrence is low at around 1% [1]. However, it may potentially be a marker of slightly increased risk for urothelial neoplasm, and a large case series showed that 1% of patients with IPB had subsequent urolethial carcinoma of the urinary tract within a mean of 27 months after surgery [2]. It has been suggested that rigorous serial surveillance cystoscopy is indicated for patients with IPB, but long-term surveillance may not be necessary for patients who had a complete resection and no previous or concurrent urothelial malignancies are documented [2]. The plan for our patient is clinical follow-up with cystoscopy.
CONCLUSION
Here we report a case of interest where an IPB at bladder neck caused intermittent urinary retention. The tumor was removed successfully and patient’s symptoms were alleviated.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}