





Abstract
Pectus excavatum is a chest wall deformity that results in caved-in or sunken appearance of lower half of anterior chest. Surgical treatment is favored when functional or cosmetic concerns arise. We present a case and series of six patients (mean haller index: 4.28) who had repair with minimal pleural disruption and sternal plate. After a broad bilateral inframammary skin incision, the anterior aspect of sternum is identified and incised. Next, the surgeon hyperextends and fixates the bone in its desired position by applying manual dorsal pressure through a small intercostal incision. Superior and inferior fasciocutaneous flaps are raised and then advanced to reconstruct the soft tissue defect. All patients had durable repair of the chest wall abnormalities and they had minimal pain during the postoperative period. No analgesia medication was necessary 1 month post-operatively. This may provide significantly less pain compared to the Nuss or Ravitch procedures to fix Pectus excavatum.
INTRODUCTION
Pectus excavatum is a chest wall deformity characterized by depression of the sternum and lower costal cartilages. The condition results in a caved-in or sunken appearance of the anterior thorax that is usually present at birth but other times develops at puberty. Surgical treatment is appropriate for patients with cardiac or pulmonary compromise or significant concern about appearance. Additionally, patients with a Haller Index (a computed tomography ratio of transverse thoracic diameter to anterior–posterior thoracic diameter) >3.25 are generally considered good surgical candidates [1, 2].
We utilized a sternal plating system to develop a modification of the Ravitch technique [3]. Our procedure results in rigid fixation of the sternum and only disrupts the pleura enough for a finger to move the sternum up. Our procedure reduces postoperative pain as it involves less constant pressure on the sternum when compared to the Nuss and only a single osteotomy when compared to the Ravitch. We were able to use our technique to successfully treat six patients at our institution.
CASE REPORT
We present a 27-year-old male who presented to clinic with a lifelong history of pectus excavatum. Initially as a child, he was asymptomatic, but over the last several years, he had begun developing shortness of breath and chest pain secondary to his pectus (Fig. 1A). On pre-op CT his Haller Index was 4.2 (Fig. 1B). It was recommended that the patient undergo repair based on his symptoms of shortness of breath and chest pain with mild exertion.
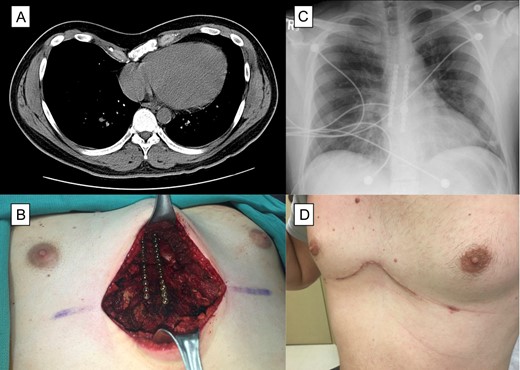
Patient with pectus excavatum. (A) Computed tomography of the patient with pectus excavatum. (B) Intraoperative view after correction of pectus excavatum and placement of sternal plates. (C) Chest X-ray after surgery showing the two sternal plate. (D) Photograph of the chest at 1 month follow up visit.
An inframammary incision is made horizontally crossing the mid sternal line. Next, broad based fasciocutaneous flaps are created superiorly and inferiorly from the manubrium to the epigastric area of the abdomen. The rectus abdominal muscle is elevated from the costal cartilages. Laterally dissection continues to directly over the medial portions of the pectoralis muscles. Bilateral pectoralis muscle flaps are raised. At this time, the manubrium, sternum, xiphoid and cartilage attachments to the structures are exposed. Deformed cartilages on both sides of the lower half of sternum and xiphoid process are removed while carefully preserving the posterior periosteum. Next, a single sternal osteotomy is performed at the greatest abnormal angle of the sternum with a saw. A small incision is made in the intercostal muscle in the fifth intercostal space above a rib just large enough for a finger to enter the pleura. At this time a single finger is used to deliver the sternum into the desired position with slight hyperextension. The sternum is secured with a titanium locking reconstruction plate (Synthes Sternal Fixation System, DePuy Synthes, West Chester, PA). The perichondrium is closed over the cartilage. The rectus abdominus is advanced and secured to the reconstruction plate as well as to the costal cartilages. The pectoralis major flaps are advanced inferiorly and toward the midline where they further correct the concave defect in the region. A chest tube was placed in the right chest. Two blake drains are inserted; one superficial to and one deep to the pectorals major flaps. A layered closure is performed.
Chest tube was removed on post-op Day #3. Both drains were removed prior to discharge. The patient was discharged home on post-op Day #4, with pain well controlled on oral pain medications. At his 1 month post-op visit patient was doing well without recurrence (Fig. 1C and D).
We performed this operation in six patients. The average age of the patient was 25 years old (range 18–39). They all presented with shortness of breath and two also presented with chest pain. The average haller index was 4.28 (3.25–5.58) on CT of chest prior to surgery. Overall the patients did well post-operatively. Only one patient had a complication where chest tube was removed after surgery but the patient later required a pigtail placement. The average length of stay was 5 days and none of the patients had recurrence. They were all off of narcotics pain medication 1 month after surgery and they all had resolution of their symptoms.
DISCUSSION
For the initial skin incision we endorse using a horizontal inframammary technique to improve scarring as it is in line with the natural skin tension lines. Invading the pleura focally at one location may reduce the chance of pneumothorax and allow us to remove chest tubes sooner. Saxena [4] describes a technique in pediatric patients where no pleura is violated and he is able to complete the operation without any chest tubes. Fonkalsrud reports being able to remove all chest tubes within 24 h of surgery with minimal occurrence of pneumothorax. In his technique he violates the pleura then makes a connection to the retrosternal space [5]. In our case series we have not found this to be the case as we had one patient to have a pneumothorax when the chest tube was pulled on post-op Day 2.
A variety of fixation systems for fixation of the sternum in pectus patients have been described including the use of absorbable plates or using mesh as a hammock [5]. Schulz-Drost et al. [6] recently published a series of 20 re-do pectus patients where they fixated the sternum using Matrix Rib titanium plates. Nazerali et al. [7] described a case series with rigid fixation of the sternum that included four pectus patients. Both of these papers showed good results. Our study focuses on the adult population and includes only primary repairs.
Outside of the pectus literature, sternal plating has been shown to improve sternal stability and provide superior bone healing [8]. We believe the use of a titanium rigid fixation system is feasible in adults because of the reduced risk of creating restrictive thoracic dystrophy in this patient population.
We present a novel technique for the correction of Pectus Excavatum utilizing the sternal plates and a minimal pleural dissection technique that has shown to be a viable option without recurrences in our series of patients. We believe rigid fixation and minimal pleural dissection will improve rapid bone healing with decreased rates of malunion, nonunion and infection.
CONFLICTS OF INTEREST STATEMENT
None of the authors, nor their close family members, have a financial interest in any of the products, devices or drugs mentioned in this article. Furthermore, the authors declare that no commercial associations or financial disclosures exist that might pose or create a conflict of interest with information presented in this manuscript. No funding was received for the work presented in this article. M.P.K. has consulted for Boston Scientific, Medtronics, Olympus and Intuitive Surgical. E.Y.C. has consulted for Boston Scientific, Medtronics and Olympus.
ETHICAL CONSIDERATIONS
The work described in this article was approved by our institutional review board. The authors adhered to the Declaration of Helsinki at all times.
ACKNOWLEDGEMENTS
None.

{kind=link}