





Abstract
Lymphangioma is a benign mass lesion characterized by numerous thin-walled lymphatic spaces that usually manifests in the first few years of life. They generally appear in the head, neck and axillary regions. Abdominal lymphangiomas have been reported however they are rare 5%. The small bowel mesentery lymphangioma has been described in <1%. Lymphangiomas may remain asymptomatic or present with complications depending on the size and location of the lesion. We present a case of a 71-year-old female, she presented to the emergency with acute abdomen and a palpable mass in the lower abdomen. Computed tomography confirmed a mass within the mesentery of the small bowel. Laparotomy was performed and a cystic mass near the root of the small bowel mesentery was found. Patient underwent full recovery. On follow-up controls, pathology described lymphangioma cavernous.
INTRODUCTION
Lymphangiomas are rare benign tumors that are formed by vascular malformations [1], they are thought to develop as a result of a failure of communication of lymph sacs with the venous drainage system [3]. They occur mainly in pediatric patients in the first few years of life [4]. They are usually located in the neck and axilla 95%, <1% affects the mesentery, greater omentum and retroperitoneum. Clinical spectrum of presentation varies from asymptomatic patients to patients resembling acute abdomen [1, 2].
We report a case of a 71-year-old female patient that arrived at the emergency room with acute abdomen, clinical examination found a palpable mass in the lower abdomen. Laboratory exams were normal and CT confirmed a mass on the mesentery of the small bowel.
Laparotomy was done and a cystic mass was found in the mesentery. The postoperative course of the patient was uneventful. On follow-up controls, patient was completely asymptomatic.
However, pathology reported lymphangioma cavernous.
CASE REPORT
Patient is a 71-year-old female, with past medical history of cholecystectomy, appendectomy and hysterectomy, she presented to the emergency department with nausea and lower abdominal pain. Having experienced 1 month of asthenia and weight loss. On clinical examination abdominal tenderness, and a lower abdominal mass was discovered.
She had normal blood work, and a contrast-enhanced abdominal computed tomography (CT) revealed a 9 × 7 × 4 cm3 mass within the small bowel mesentery near the root of the mesentery with several lymph nodes surrounding it. No other lesion or masses were found (Fig. 1A).
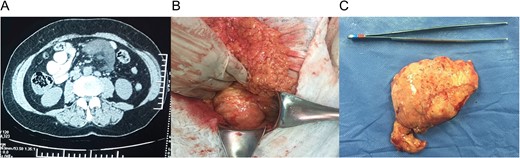
(A) Computed tomography (CT) with a 9 × 7 × 4 cm mass within the small bowel mesentery near the root of the mesentery. (B) Mass in the root of small bowel mesentery near the mesenteric vessels. (C) External surface of the mass.
With these findings, surgery was decided and at laparotomy, a 9, 5 × 7 × 5 cm3 mass was discovered in the root of small bowel mesentery, near but not in contact with major vessels, it was completely resected with a 0.5 cm margin, respecting bowel wall and vessels (Fig. 1B).
The external surface of the mass had a yellowish like-fat aspect and contained white milky fluid, the mass contained some cystic lesions and the wall was 0.5 cm in width (Fig. 1C). Pathology reported encapsulated fat tissue surrounded by dilated lymph vessels that contained lymphocytes. Immunohistochemical study for D2-40 was positive. Lymphangioma cavernous was the final diagnostic (Fig. 2A–C).
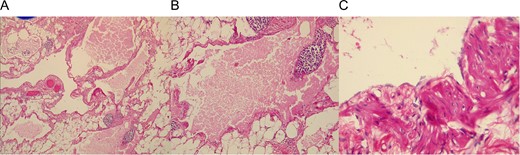
(A) Adipose tissue covering lymphatic vessels with eosinophil content. (B) Dilated lymphatic vessel with a cluster of lymphocytes. (C) Cyst epithelium.
The postoperative course of the patient was uneventful, she initiated soft diet a day after surgery and was discharged once full diet was resumed.
On follow-up controls, patient was completely asymptomatic, without any pain or complications.
DISCUSSION
Lymphangioma is a rare benign intra-abdominal anomaly with uncertain etiology, predominantly occurring in children [2], adult cases are rare [1, 5, 6] they predominantly appear on the neck, head and axillary regions. They can also appear in the abdominal or mediastinal cavity however they are rare, among this lymphangioma of the small bowel mesentery has been described in <1% of lymphangiomas [1].
Lymphangiomas are thought to develop as a result of a failure of communication of lymph sacs with the venous drainage system [3]. However, other etiologies have been described and may occur after abdominal trauma, lymphatic obstruction, inflammatory process and surgery [2]. Our patient had previous surgeries that may have contributed to the development of this tumor since no masses were ever described in previous surgical interventions.
Lymphangiomas are traditionally classified into three histologic types: capillary, cavernous and cystic [1], the clinical symptoms of a mesenteric lymphangioma are non-specific and may include abdominal pain, vomiting, abdominal distension, a palpable abdominal mass or acute abdomen. Diagnosis is practically impossible on clinical grounds [1, 3]. The differential diagnosis includes a wide range of cystic intraabdominal lesion ranging from abdominal lymphoma, secondary metastasis from an unknown primary, tuberculosis, hydatid disease, small bowel adenocarcinoma, to rare mesenteric tumors; including desmoid, schwannomas, smooth muscle tumors and sarcomas [3, 4]. Images studies like echography or tomography may give clinical orientation, however, the final diagnostic is given by pathology [7].
Our patient did not have a history of pancreatitis to suggest pseudocysts, abdominal tuberculosis and malignancy could not be excluded since she had a history of the weight loss. However, since she arrived with nausea, a mass in the abdomen, and sudden lower abdominal pain, with tenderness. She required a diagnostic laparotomy to reach a final diagnosis
Primary treatment of lymphangiomas is radical surgical excision even when asymptomatic for its potential to grow enormously to invade adjacent structures, develop complications and has a risk of sarcoma transformation on irradiation [5], incomplete resection usually leads to recurrence in ~10–15% [7], however, sometimes it can be challenging, even impossible, to respect the cyst completely due to adhesions with the surrounding structures [4]. In our case intraoperative decision making was straightforward. The lesion looked benign and we were able to achieve complete resection in view of no vascular involvement.
Lymphangiomas, prove that acute abdomen can be caused by rare pathologies, even the ones that we are not used to seeing on daily basis or age demographic. Intraoperative decision making is critical since lymphangiomas may be invasive and grow to an enormous size however they usually have a good prognosis. Surgical excision is the treatment of choice.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}