





Abstract
Introduction: Solitary fibrous tumors of the pleura (SFTP) are rare mesenchymal tumors representing <5% of all tumors of the pleura. Literature reveals only two case series and a few solitary reports. Case report: A 68-year-old male presented to our hospital after experiencing exertional dyspnea. A chest CT revealed a giant heterogeneous mass. CT-guided transthoracic core needle biopsy demonstrated SFTP. The well-circumscribed, encapsulated resected mass was measured to be 30 cm × 21 cm × 15 cm and weighed 6900 g. Discussion: SFTP are a rare pathology of the pleural cavity, which most of the time develop from submesothelial fibroblasts of the visceral pleura. Due to their non-characteristic clinical picture, SFTP are usually diagnosed in the later stages of the development. A significant issue in the management of giant SFTP is radical resection of the tumor to relieve compression of the lung parenchyma and other mediastinal structures. Conclusion: SFTP are rare neoplasms that fortunately are benign 80% of the time. Only a few cases of giant SFTP that cover almost the entire pleural space are described in the literature. This report represents one of the largest resected SFTP reports in the literature.
INTRODUCTION
Solitary fibrous tumors of the pleura (SFTP) are rare mesenchymal tumors representing <5% of all tumors of the pleura [1]. Literature reveals only two case series and a few solitary reports [2]. SFTP affect male and female patients equally; however, they may develop in all age periods (5–87 years) with the highest incidence between 60 and 70 years of age [3, 4]. Generally, there is no genetic predisposition, and in contrast with mesothelioma [5], there is no relationship to the exposure to asbestos, tobacco or any other environmental agents [6]. Most SFTP are benign, but may alter in malignancy with age. They usually develop in lower part of pleural cavity; from the visceral pleura in around 80% [6]. Individual tumors grow over 10 cm; however, only individual cases of giant tumors measuring over 20 cm are described [1]. We report a patient with giant SFTP, weighing 6900 g.
CASE REPORT
A 68-year-old male presented to our hospital after experiencing exertional dyspnea and shortness of breath for 2 months. He had no other chest complaints, such as cough, hemoptysis or chest pain. His medical history was unremarkable and he had no history of exposure to asbestos. He had no exposure to tobacco. His blood pressure was 136/78 mmHg, pulse was 92 beats/min and respiratory rate was 23 breaths/min. He was afebrile, and oxygen saturation was 94% in room air. Examination of the chest revealed dullness and diminished breath sounds on the right hemithorax. A plain chest X-ray showed a right side huge opacity (Fig. 1). A contrast-enhanced computed tomography (CT) revealed a large heterogeneous mass that almost completely fill the right hemithorax (Fig. 2a and b). CT-guided transthoracic core needle biopsy demonstrated SFTP. Under general anesthesia and with the use of a single lumen endotracheal tube, right posterolateral thoracotomy was performed through fifth intercostals spaces. Upon entering the pleura we visualize a very huge encapsulated mass with adhesion to chest wall (Fig. 3a). After adhesiolysis, the main vascular pedicle of the tumor from the upper lobe was ligated with non-absorbable suture.The well-circumscribed, encapsulated resected mass was measured to be 30 cm × 21 cm × 15 cm and weighed 6900 g in the fresh state (Fig. 3b and c). The postoperative course was uneventful and the patient was discharged on postoperative Day 6. The patient is currently alive without any recurrence twelve months after the surgery. The histological findings revealed spindle tumor cells arranged with varying amounts of collagen and hyalinization of fibrous tissue (Fig. 4a). Mitosis was rarely present. Immunochistochemically tumor cells were reactive for CD34, and bcl2 and typically no immunoreactivity was observed with S-100, WT-1, Desmin, CEA, CK AE1/AE3, CK5/6 and calretinin (Fig. 4b and c). According to the morphology and cellular immunophenotype the diagnosis of benign giant pleural SFT was signed out.

Chest radiography showing a large opacity in the right hemithorax.
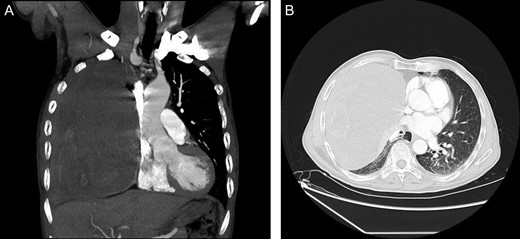
(A and B) Contrast-enhanced CT showing a very large heterogeneous mass in the right hemithorax.
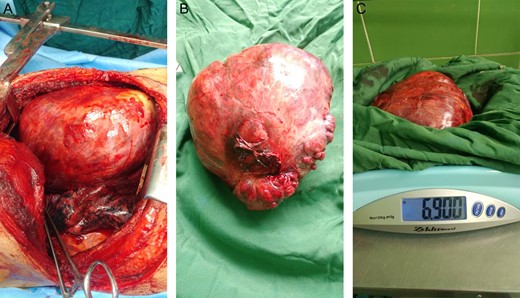
(A–C) Large encapsulated mass.
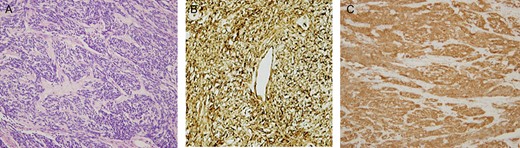
(A–C) Light microscopy of the resected tumor (H&E stain) revealed patternless spindle tumor cells mixed with varying amounts of collagen, and hyalinization of fibrous tissue (A). Positive immunoreactivity of tumor cells. CD34 (B) and BCl2 (C).
DISCUSSION
SFTP are a rare pathology of the pleural cavity, which most of the time develop from submesothelial fibroblasts of the visceral pleura [6]. Due to their non-characteristic clinical picture, SFTP are usually diagnosed in the later stages of the development, when causing pressure on the surrounding structures on account of their size [1]. Larger tumors, more than 10 or 15 cm in diameter, occupying a larger space, and compressing other thoracic structures, may cause symptoms such as dyspnea, chest pain, cough and fatigue [7, 8]. A confident pre-operative diagnosis of a fibrous tumor of the pleura can be made by histologic and immunohistochemical analysis of material obtained by transthoracic Tru-Cut needle biopsy. Smaller, accidentally discovered SFTP are relatively easy to remove surgically. A much more significant issue are radical surgical procedures of giant SFTP in patients affected by the pressure of the tumor on the mediastinal structures and lungs. Only a few cases of giant SFTP that cover almost the entire pleural space are described in literature. Certain authors report of having performed the surgery via one or two thoracotomies at two different levels [1], others via sternotomy [9]. Our approach via right posterolateral thoracotomy provides an optimal view of the pleural cavity. In this case the tumor was very huge with weighed 6900 g. SFTP that we resected belongs to the largest so far described cases in global literature. It is possible that the tumor will recur, which mainly depends on the histological characteristics of SFTP and radical nature of the surgical procedure. The possibility of benign pedunculated tumors recurring is around 2%, for benign sessile tumors around 8%, malignant pedunculated tumor around 14%, and for malignant sessile tumors around 63% [10, 11]. It is necessary to follow the patients. Postoperative surveillance with CT imaging every 6 months is recommended.
CONCLUSION
SFTP are rare neoplasms that fortunately are benign 80% of the time. Only a few cases of giant SFTP that cover almost the entire pleural space are described in literature. SFTP that we resected belongs to the largest so far described cases in global literature. They are readily curable with careful, complete resection. Although the less common malignant variety of SFTP has a higher recurrence rate and higher tumor-related mortality, aggressive surgery and careful postoperative surveillance may still permit long-term survivals in as many as 70% of these patients. Surveillance is required post-operatively to detect recurrence.
ACKNOWLEDGEMENTS
Thanks to anesthesiologist of Valiasr Hospital.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}