





Abstract
Ectopic lingual thyroid has been described, however, follicular carcinoma arising within it is an extremely rare entity with only 40 cases reported in the literature. Lingual thyroid carcinoma is undistinguishable from benign enlargement of lingual thyroid, the later should also be differentiated from many oropharyngeal pathologies including but not limited to thyroglossal duct cyst, lipoma, dermoid cyst and salivary gland tumors. Ectopic lingual nature of thyroid tissue can be diagnosed with scintigraphy scan; however, malignant transformation confirms just after pathological examination. Surgical excision remains the best therapy with transoral approach being the most appropriate and favorable among others due to its cosmetic results and lower incidence of infection. Herein, we report a case of an adult female who was diagnosed to have follicular carcinoma of an ectopic lingual thyroid tissue mass. Concerning the size of the mass it was the largest of all reported cases of ectopic thyroid gland.
INTRODUCTION
Ectopic thyroid tissue is defined by the presence of thyroid tissue anywhere along the path drawn between the foramen cecum and its normal anatomic location in the neck [1]. Lingual thyroid gland results from failure of the thyroid tissue to migrate from the foramen cecum. There are around 400 reported cases of ectopic lingual thyroid glands [2]. Undiagnosed lingual thyroid remnants are present in around 10% of people as demonstrated by postmortem studies [3]. Carcinoma arising from a lingual thyroid tissue is even amore rare entity with a rate of 1% having follicular carcinoma as the most common histopathology unlike that encountered in orthotopic thyroid and thyroglossal cyst which is mainly of the papillary type [4].
CASE REPORT
We report a case of a 32-year-old-lady who presented to our department complaining of dyspnea, dysphagia, hot potato voice and decreased appetite. Her symptoms exacerbated as she got pregnant 4 years prior to presentation. Her medical and surgical records were unremarkable. Physical examination disclosed a large, incompressible, non-tender midline mass at the base of the tongue extending posterio-inferiorly. Fibroptic nasolaryngoscopy demonstrated extension of the mass down to the valleculae with a wide base and an eventual narrowing of the hypopharynx. Blood tests were strictly normal except for hypothyroidism (TSH 18 uIU/dl, FT4 0.85 pg/dl). Computed tomographic (CT) scan depicted a large enhancing, homogeneous and well demarcated mass at the tongue base region (Fig. 1). Scintigraphy scan revealed increased uptake in that region confirming the ectopic lingual nature of thyroid tissue. Patient was scheduled for complete surgical resection after she rendered euthyroid. By adopting the external cervical approach, a midline mandibular split combined with lateral pharyngotomy provided adequate exposure and good bleeding control during the operation. Then en-block resection of the mass performed (Fig. 2). Postoperative course was uneventful. On pathological examination the specimen weighed 32 g and measured 6.0 × 4.0 cm2. Microscopically, the nodule revealed to be a minimally invasive follicular carcinoma arising in a lingual ectopic thyroid tissue (Fig. 3). Patient received radioactive I 131 as a complementary treatment. Follow up after 6 months revealed a firmly normal examination.

Axial computed tomography-scan with contrast showing a large 6 × 4 × 3.5 cm3 lingual tumor (black arrow).
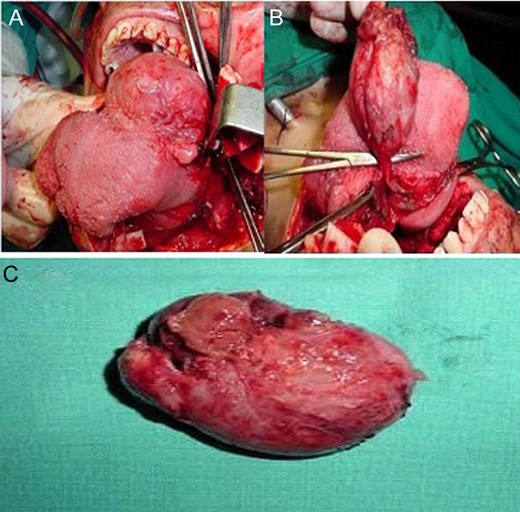
Open approach with mandibular split (A), en-block resection of the lingual thyroid (B), final specimen (C).
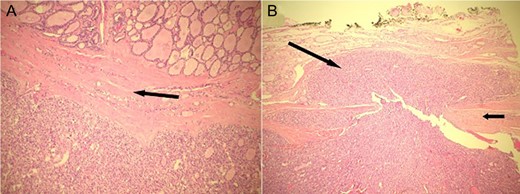
(A) The nodule shows a microfollicular and trabecular architecture (lower part). It is well demarcated from the lingual thyroid tissue (upper part) by a fibrous capsule (arrow). (B) A mushroom-shaped throng of neoplastic follicular cells (long arrow) is seen invading through the capsule (short arrow).
DISCUSSION
Ectopic thyroid gland is an infrequent disorder resulting from a defect in the embryological development, with location being mostly at the tongue base. In 1869 Hickman W. described first case of carcinoma in ectopic lingual thyroid [5]. So far there are only 40 reported cases in the literature (10% of lingual thyroid). Although the predominant subtype of lingual thyroid carcinoma has been follicular carcinoma, the more recent studies have reported several cases of papillary carcinoma in ectopic lingual thyroids [5]; rarely hürthle cell and medullary thyroid carcinoma [4, 6, 7].
The differential diagnosis of a mass at the base of tongue is extensive including lingual thyroid, thyroglossal duct cyst, lymphangioma, fibroma, lipoma, hypertrophied lingual tonsillar tissue, hypertrophied seromucinous gland, dermoid cyst, papilloma, squamous cell carcinoma, verrucous carcinoma, thyroid carcinoma, minor salivary gland tumors and lymphoma [1, 7]. On clinical basis, it is hard to differentiate lingual thyroid carcinoma form a symptomatic lingual thyroid. However, rapid growth or ulceration may suggest development of carcinoma. The most common symptoms include dyspnea, voice change or foreign body sensation [6, 8].
Initial diagnostic modalities include radionucleotide scans using I 123, I 131 or T 99 m [1, 3]. Uptake of radionucleotide within the tongue confirms the presence of ectopic thyroid tissue; moreover, simultaneous survey of the neck typically demonstrates the absence of activity. CT also accurately outlines the extension of the mass as well as it defines the adjacent structures. Magnetic resonance imaging remains the preferred non-invasive imaging technique because of its ability to provide enhanced soft-tissue definition and multiaxis imaging [7, 9].
Owing to the rarity of this entity, no consensus has been made regarding the most appropriate treatment. However, surgical excision with wide margins is the first line therapy. Several surgical approaches have been described for excision: transoral, external approaches like transhyoid, lateral pharyngotomy with or without mandibular split. However, good exposure and control of bleeding from lingual arteries remain the main factors that determine the most appropriate surgical approach. Most of the reported lingual thyroid glands were excised using the transoral approach [10], benefiting from its favorable cosmetic outcome; and a relatively low incidence of postoperative infection as well as a shorter hospital stay. On the other hand, large masses are poorly expose and lingual arteries are hardly controlled [10]. In comparison, the external approach offers good visualization particularly for large masses with the possibility of neck dissection [7].
In conclusion, we believe that the sizes of the masses reported in the literature were not so large and therefore the transoral approach was sufficient for an acceptable exposure. Owing to the large dimension of the ectopic thyroid gland in the current case, we found that an external approach is the safest for accomplishing total resection. In this paper we have clearly demonstrated that the size of the lesion played a crucial factor in deciding which approach was most suitable. Concerning the size of all the reported ectopic thyroid glands, our case presents the largest dimension 6 × 4 × 3.5 cm3.
CONFLICT OF INTEREST STATEMENT
The authors declare that there is no conflict of interest, financial or otherwise, related to the publication of this study or its findings.

{kind=link}
{kind=link}
{kind=link}