





Abstract
Teratomas are tumors composed of tissues derived from more than one germ cell line. They manifested with a great variety of clinical and radiological features. We report a case of a giant left hemithorax teratoma in a female with huge spleen tumor and review the relevant literature. A 38-year-old female with progressively aggravating dyspnea at rest from a mild trauma. Absent breath sounds on the left side. There was splenomegaly. Computed tomography scan revealed a huge mass (20 × 15 × 18 cm), containing elements of heterogeneous density in the left hemithorax. The spleen tumor was occupying most of the spleen without any other abdominal manifestations. The patient underwent left thoracotomy and laparoscopic splenectomy. Histopathological examination revealed a benign mature teratoma and cystic lymphangiomatosis of the spleen. To the best of our knowledge and after reviewing the available literature this is the first case of huge mature pulmonary teratoma with large cystic spleen lymphangiomatosis.
INTRODUCTION
Teratomas are the most common germinative cell tumors. They originate from multiple germ cell lines of tumors, primarily in the gonads and represent the most common mediastinal masses—especially in the anterior mediastinum, which is the most common extra-gonadal manifestation [1]. Intrapulmonary teratomas are rare and were first acknowledged by Dr Mohr in 1839 [2]. Teratomas, may exhibit a variety of presentations and radiological findings. Cystic lymphangiomatosis of the spleen is very rare but benign due to a congenital malformation of the lymphatic system [3].
CASE REPORT
A 48-year-old Palestinian female patient with a history of trauma. The patient had slipped and fallen on her upper back, and she complained of progressively aggravating dyspnea at rest. Then, within the chest x-ray of trauma survey, found an incidentally huge mass occupying the left lung, irrelevant to the trauma. There was no past medical history, and the only surgical history consisted of one cesarean section 3 years prior to the visit. The patient was married and had four children. She was a non-smoker and had no recent history of traveling, weight loss or expectoration.
Examination showed that the patient was stable with mild tenderness on palpation of the posterior upper back. Auscultation demonstrated absent breath sounds on the left. An abdomen examination concluded that there were splenomegaly.
Chest x-ray showed well-defined huge opacity of most left hemithorax with a shift of mediastinum to the right (Fig. 1). CT chest/abdomen/pelvis with IV contrast revealed 20 × 15 × 18 cm3 well-defined mixed cystic lesion within the left lung containing multiple parts of the heterogeneous density with soft tissue elements and fat content. It also showed spots of wall calcification, where the lesion probably originated from the mediastinum, involving most of the left hemithorax. The mass compressed the mediastinal structures, great vessels, and airways (Fig. 2). It is surrounded by a consolidation collapsed with a marked shift of mediastinum to the right side (Figs 2 and 3). No mediastinal lymphadenopathy and the right lung was clear. The spleen was enlarged with multiple cysts that varied in size with no significant enhancement post IV contrast in arterial and portal phases (Figs 2 and 4). The liver was unremarkable. Hematological tests were within normal limits. Mantoux test and Sputum culture were negative.
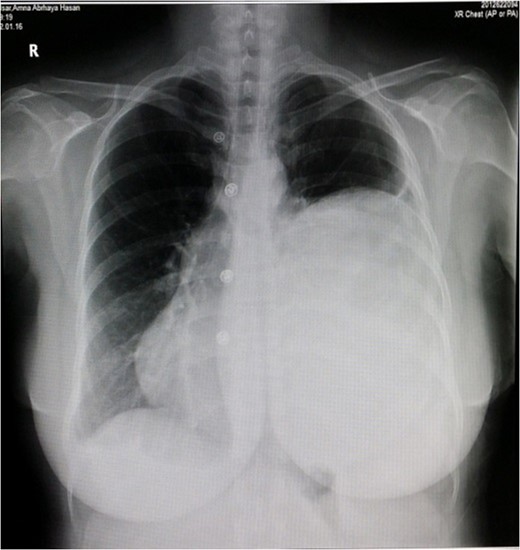
X-ray of the chest.
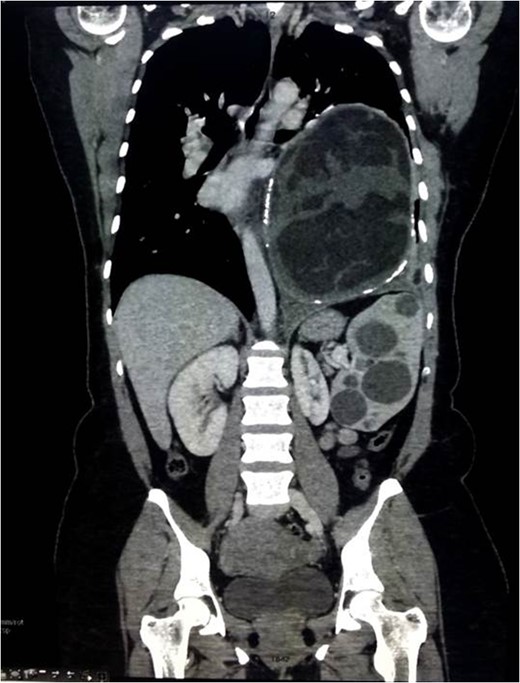
Coronal view of CT scan of the chest/abdomen/pelvis.
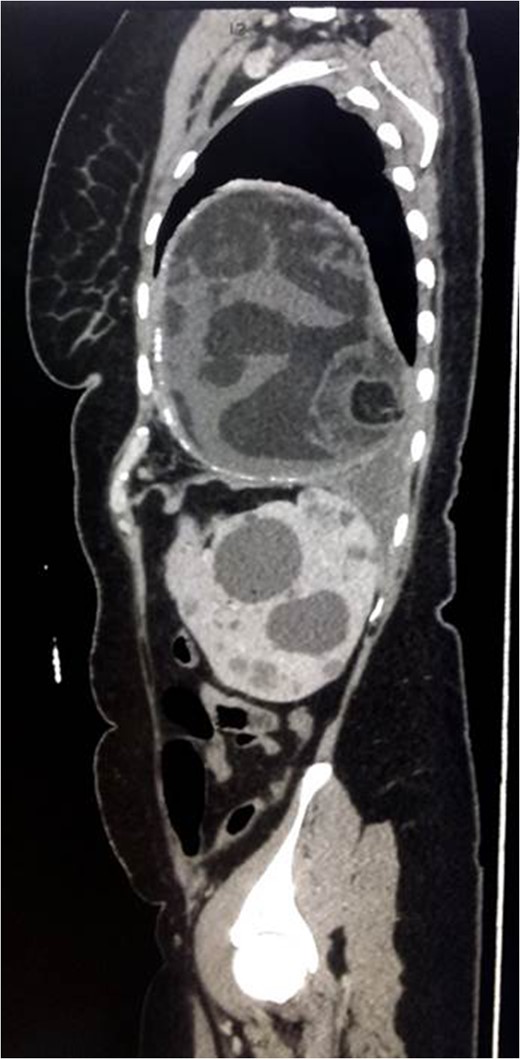
Sagittal view of CT scan of the chest/abdomen/pelvis.
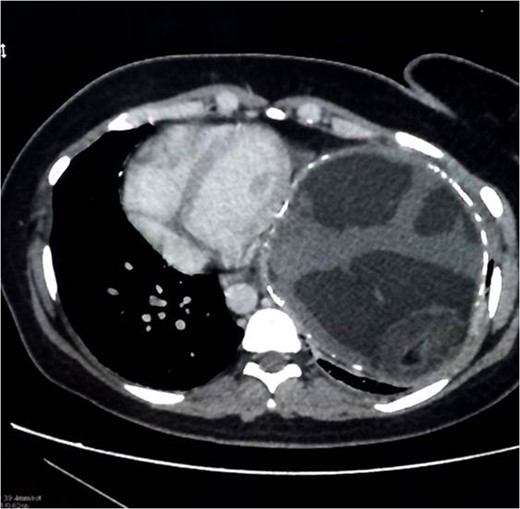
Axial view of CT scan of the chest/abdomen/pelvis.
The decision was to perform a standard left anterolateral thoracotomy to remove the thoracic tumor after expiration because the cystic tumor was found to be very congested and vulnerable to rupture during the extraction (Fig. 5). It emptied a large amount of thick, white/yellowish fluid and hair particles (Fig. 6). The size of the tumor was extremely large, although no invasion to the mediastinum, vessels or to the airway had occurred. The tumor detached from the phrenic angle, diaphragm and all of the surrounding structures without any bleeding, air leak or complications. A laparoscopic splenectomy was done in the same session, and the spleen was extracted through the old cesarean incision scar for cosmetic purposes; the spleen shows multiple cysts on both visceral and diaphragmatic surfaces (Figs 7 and 8).
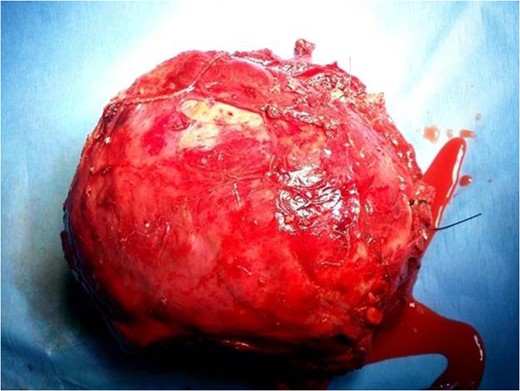
Teratoma sac after aspiration and removal from the thorax with noted hair particles.

Aspirated fluid from the teratoma sac.

Visceral surface of the spleen with noted multiple masses.

Diaphragmatic surface of the spleen with multiple masses.
The patient was discharged on the 5th postoperative day. Histopathological examination revealed numerous fluid with soft tissue, squamous epithelium, adipose tissue, hair particles and calcification at the wall, which suggests benign mature intrapulmonary teratoma. The spleen contained multiple cysts that varied in size with mural calcification, which suggests cystic lymphangiomatosis of the spleen. The patient showed a good response in the follow-up with normal vital signs and labs.
DISCUSSION
Teratomas are the most common type of germ cell tumors. These tumors are primarily found in the gonads, and a common mediastinum tumor presents in the anterior mediastinum predominantly accounted for ~80% of mediastinal teratomas, The most specific sign for teratoma in the lung is trichoptysis (expectoration of hair) [1]. Pulmonary teratomas are commonly cystic and of a mature type, and usually range in diameter from 2.8 to 3 cm [4]. Diagnosis of the patient usually begins with a regular chest x-ray followed by a CT scan of the chest. CT imaging is used to estimate the accurate size of the tumor, and the density of each element is presented in the cyst, such as soft tissue, liquid tissue, fat, teeth and calcification, and the presence of fat to liquid level is greatly specific to diagnose teratoma initially [5]. MRI is considered best to distinguish the anatomic relation to the mediastinum, hilum of the lung and vessels [6]. Teratomas are accurately diagnosed by microscopic examination, and generally, teratomas are classified into mature teratoma, which is well differentiated with three or at least two tissues derived from germ cell lines as well as immature teratoma, which comes with embryonic tissues, and teratomas with malignant transformation properties [7]. Mature teratoma is managed by surgical excision to prevent recurrence and rupture, especially if it contains pancreatic tissue and the prognosis in teratoma of a mature type is excellent after excision [5].
Lymphangiomatosis is multiple lymphangiomas with a cystic nature, usually a slowly growing benign tumor, due to congenital dilatation of the lymphatic system rarely found in the spleen; it affects children and has a female preponderance, and it is typically discovered incidentally as a rare differential diagnosis of massive splenomegaly [3]. CT is the best method to diagnose and identify the presence of mural calcifications [8]. The best management of the patients is complete surgical resection with good prognosis after resection. The main complication after surgery is recurrence reported in about 10%, usually due to incomplete resection [9].
CONCLUSION
Splenic lymphangiomatosis should be considered in the massive splenomegaly differential diagnosis. To our knowledge and after reviewing the available literature, this is the first case of a huge mature pulmonary teratoma with large cystic lymphangiomatosis of the spleen. Complete resection of the teratoma showed a good response from the patient. The laparoscopic splenectomy was very helpful to achieve a fast recovery.
FUNDING
None declare.
CONFLICT OF INTEREST STATEMENT
None declare.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}