





Abstract
Colorectal carcinoma is common worldwide and its metastasis represents the main cause of mortality related to the disease. Inguinal metastization of this tumor has been considered almost impossible, owing to colon anatomy and its cranial lymphatic drainage. We report the case of a 63-year-old man submitted to laparoscopical sigmoid colectomy, due a sigmoid adenocarcinoma. During follow-up, a right inguinal lymphadenopathy with 25 mm was detected. Fine needle aspiration biopsy revealed that it was a colon adenocarcinoma metastasis, and thus the patient underwent an inguinal lymphadenectomy. The histological study confirmed metastatic adenocarcinoma of the colon and the patient was submitted to 5-fluouracil and oxaliplatin chemotherapy. This case coursed with metastasis to the right inguinal region; although, the pathophysiological mechanism involved is difficult to understand. There are no solid data for the management of these patients. Inguinal lymphadenectomy and chemotherapy, proved to be effective.
INTRODUCTION
Colorectal carcinoma is a common neoplasm worldwide [1]; for these patients, the presence of metastases represents the main cause of mortality related to the disease [2]. Considering that, ~25% of patients have metastases at the time of the initial diagnosis, and that almost 50% of patients with colorectal carcinoma will develop metastatic disease, the mortality rate of this tumor is high. At 5 years, the mean survival rate for colorectal carcinoma is ~60% [3].
In a metastatic colorectal carcinoma, metastases are usually limited to a single area, the liver and lungs being the most commonly involved organs [4]. Although unusual, metastization to other organs, such as breast and thyroid gland has been sporadically reported in literature.
In respect to inguinal lymph node involvement, from colon carcinoma spreading has been considered almost impossible, due to the anatomical features and cranially directed lymphatic drain of the colon [5].
Therefore, the aim of this study was to describe a rare case of right inguinal metastasis of an adenocarcinoma of the sigmoid colon.
CASE REPORT
A Caucasian man 63-year-old, was referred to the hospital from primary care, because of constipation and defecatory difficulty (needed more effort), with 2 months of evolution. His family history was unremarkable and he was previously healthy.
From the study carried out, colonoscopy revealed a vegetated and ulcerated lesion, with 35–40 mm, in the sigmoid colon at 45 cm from the anal margin; and thus, biopsy and tattoo of the lesion was simultaneously done. Once pathology revealed an adenocarcinoma of the sigmoid colon and the thoraco-abdomino-pelvic computerized tomography (CT) excluded the existence of secondary lesions, surgical treatment was proposed to the patient, who consented to the treatment plan that was offered.
He was submitted to laparoscopical sigmoid colectomy with no complications; intra-operatively there was no evidence of peritoneal carcinomatosis, ascites or hepatic lesions. The pathology examination of the surgical specimen showed a moderately differentiated adenocarcinoma; and of the six lymph nodes isolated, none of them had evidence of metastasis. The tumor size was 2.8 × 1.5 × 0.5 cm3, sparing the surgical margins. Therefore, it was assigned a pathological staging pT2N0M0 and the Multidisciplinary Oncology Group decided to just keep surveillance.
The patient remained in follow-up for 2 years with no evidence of recurrence by CT and colonoscopy. After 2 years, endoscopic evaluation became impossible due to stenosis of colorectal anastomosis (not transposable), requiring the realization of colonography by CT to exclude external compression of the anastomosis. The test showed absence of expansive lesions around the anastomosis, polypoid thickness or abnormal parietal thickness, although it revealed a right inguinal lymphadenopathy with 25 mm (Fig. 1), deserving histological characterization. Fine needle aspirative biopsy concluded that the new lesion represented a colon adenocarcinoma metastasis.
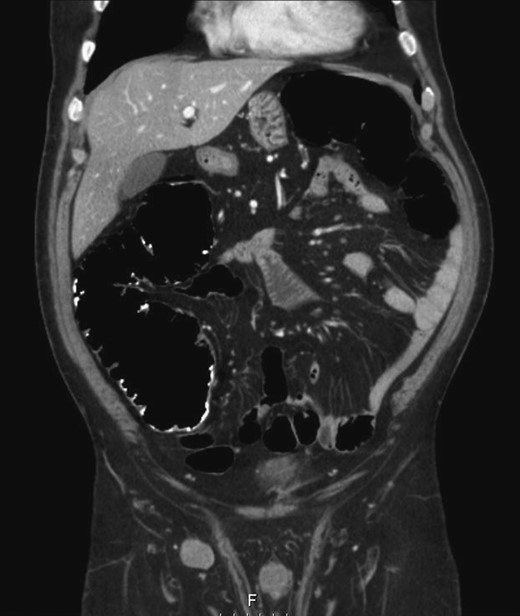
Right inguinal lymphadenopathy in colonography by computerized tomography.
He was then submitted to inguinal lymphadenectomy and the definitive histological study confirmed, from six isolated nodes, one with metastatic adenocarcinoma of the colon. According to this, the Multidisciplinary Oncology Group decided to proceed to adjuvant chemotherapy with leucovorin, 5-fluouracil and oxaliplatin (FOLFOX).
At the time of this report, ~1 year following all treatments, there is no evidence of disease recurrence.
DISCUSSION
This is a case of left colon cancer (sigmoid) with metastasis for the right inguinal region it being difficult to understand the pathophysiological mechanism involved in this phenomenon. A possible explanation would be via liver metastization, with consequent umbilical metastasis via portal system, and subsequently occurrence of the inguinal metastasis through the abdominal wall lymphatics [6]. Another explanation would be the occurrence of intra-abdominal spread of the primary lesion, with progression over the iliac vessels to the inguinal nodes [7]. However, there were no imagiological signs of other lesions, particularly in the liver, neither intra-operative evidence of spread. Therefore, the explanation provided above were excluded for the nature of the metastasis in this case, making it even rarer and scientifically curious.
Doing a retrospective analysis of the therapeutic approach, we can ask whether the patient should have been a candidate for adjuvant chemotherapy. According to the European Society for Medical Oncology Consensus Guidelines [8] it is recommended for stages ≥pT3b and/or N+, and the present case is a pT2N0M0 stage. However, from the same consensus, patients with more than 60 years and low number of lymph dissected nodes should perform adjuvant chemotherapy [8], and the patient has 63-year-old and six lymph nodes were isolated.
Furthermore, high-risk characteristics are considered: lymph node sampling <12; poorly differentiated tumors; vascular, lymphatic and perineural invasion; presentation of tumor obstruction or perforation and tumor stage pT4 [9]; corroborating that, since six lymph nodes were isolated, the adjuvant chemotherapy could have been considered.
There is no solid scientific evidence to support the therapeutic decisions for an atypical presentation of a sigmoid adenocarcinoma; although, we must keep in mind that the chosen treatment should increase the survival with low morbidity for the patient [10]. In this case, after the spreading, it was decided to perform inguinal lymph node dissection followed by adjuvant chemotherapy. We have a short follow-up after the last intervention, but to date, there is no evidence of disease recurrence.
Owing to the lack of available published experience in the diagnosis and treatment of atypical presentations of colon cancer we believe that sharing our experience we contribute to optimize diagnosis and treatment of the situations.
CONFLICT OF INTEREST STATEMENT
There are no conflict of interests to declare.

{kind=link}