





Abstract
Thymic epithelial tumors occur in 1–5% of patients with multiple endocrine neoplasia type 1 (MEN 1). Majority of these thymic epithelial tumors are thymic carcinoids and patients with thymoma in MEN 1 is rare. Furthermore, thymoma with neuroendocrine differentiation was also rarely reported. Herein, we report a 68-year-old man having type B3 thymoma with neuroendocrine differentiation in MEN 1 and to the best of our knowledge this is the first such case ever reported.
INTRODUCTION
Multiple endocrine neoplasia type 1 (MEN 1) is an autosomal dominant tumor syndrome arising from mutations of the MEN 1 tumor suppressor gene on chromosome 11q13 [1]. It is characterized by primary hyperparathyroidism, enteropancreatic neuroendocrine neoplasia and pituitary neoplasia [1].
Thymic epithelial tumors are less common (1–5%) manifestations of MEN 1 [2]. Furthermore, majority of these thymic epithelial tumors are thymic carcinoids and thymoma patients in MEN 1 is rare. Only four cases of thymoma with MEN 1 were found when we performed a literature search using PubMed [3–6].
Although thymic carcinomas often contain tumor cells having a neuroendocrine feature, thymomas with neuroendocrine differentiation are extremely rare [7, 8].
Herein, we report a case of thymoma (World Health Organization [WHO] type B3) with neuroendocrine differentiation in MEN 1.
CASE REPORT
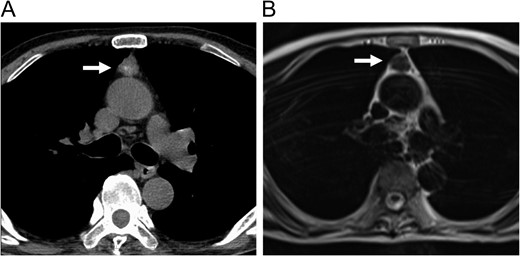
Enhanced CT (A) and MRI (B) of the chest revealed an anterior mediastinal tumor.
Surgical exploration was performed through a video-assisted thoracoscopic surgery under general anesthesia. No tumor invasion to the pericardium and lung was found. The tumor was smoothly removed. Post-operative course was uneventful.
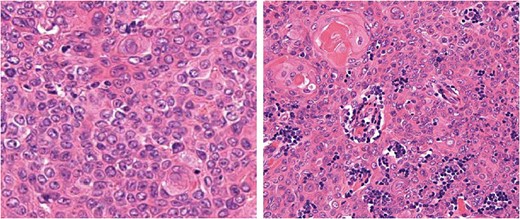
Histological findings of the tumor. Hematoxylin and eosin staining.
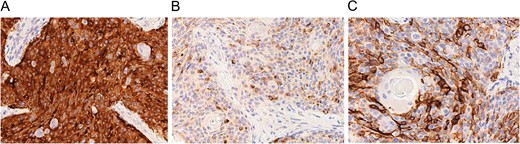
Immunohistochemical findings of the tumor for synaptophysin (A), chromogranin (B) and CD56 (C).
After surgery, his symptom (progressive muscle weakness) unchanged and he was diagnosed as amyotrophic lateral sclerosis. At six post-operative months, there was no evidence of local recurrence or distant metastasis.
DISCUSSION
The present case had two rare characteristics. First, majority of thymic epithelial tumors in MEN 1 are thymic carcinoids and patients with thymoma in MEN 1 is rare [3–6]. Second, thymomas with neuroendocrine differentiation are extremely rare [7, 8]. To the best of our knowledge, this is the first such case ever reported.
Only four cases of thymoma in MEN 1 was previously reported [3–6]. Miller et al. [3] reported a case of synchronous thymoma (type B3) and thymic carcinoid in a woman with MEN 1. Kojima et al. [4] reported a mixed-type invasive thymoma (WHO histological type was not available) with MEN 1. De Toma et al. [5] reported a thymoma (type B1) in MEN 1. Vroegindeweij-Claessens et al. [6] reported a case of myasthenia gravis and thymoma (WHO histological type was not available) in MEN 1. Vroegindeweij-Claessens et al. [6] discussed that the association of tumor of the thymus and parathyroid gland is not surprising as these structures have a common embryonic origin from the third pharyngeal pouch. This discussion is helpful to understand the association between thymic epithelial tumor and MEN 1. Lim et al. [10] examined possible genotype–phenotype correlation in thymic carcinoid from MEN 1 and reported a high prevalence of truncating MEN 1 mutation in patients with thymic carcinoid. This might be a pathways of tumorigenesis of thymic carcinoids in MEN 1 at least in part. However, it has been still unknown why thymoma in MEN 1 is rare.
The neuroendocrine differentiation of thymomas is extremely rare [7, 8]. None of previously reported four thymomas in MEN 1 [3–6] showed neuroendocrine differentiation. It has been accepted that thymic carcinomas often exhibit neuroendocrine differentiation [9]. However, reports of thymomas with neuroendocrine differentiation have been extremely rare [7, 8]. The present case is a first case of thymoma with neuroendocrine differentiation in MEN 1. Shiraishi et al. [7] reported a case of thymoma (type B3) with neuroendocrine differentiation. Park et al. [8] also reported an atypical thymoma (type B3) with neuroendocrine differentiation combined with hyperparathyroidism. Although their case did not fulfill the diagnostic criteria of MEN 1, their case might have a similar genetic background with the present case.
It has been reported that MEN 1-related thymic carcinoids carry an ominous prognosis due to their aggressive nature and potential for metastasis, and they are associated with increased mortality in patients with MEN 1 [11]. To date, it is unclear whether neuroendocrine differentiation itself is associated with increased malignancy in thymic epithelial tumors. Further, long-term follow-up of thymomas with neuroendocrine differentiation will be necessary.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}