





Abstract
We report here a rare case of primary hyperparathyroidism that was associated with an ectopic parathyroid adenoma located in the mediastinum. A 66-year-old woman suffering from primary hyperparathyroidism had been followed-up on an outpatient basis for over 10 years. She suffered from persistent urolithiasis and osteopenia due to hypercalcemia. After technetium-99-sestamibi (99mTc-MIBI) scintigraphy revealed an ectopic adenoma in the superior mediastinum, thoracoscopic resection of the tumor was performed. Subsequently, her serum parathyroid hormone (PTH) level decreased dramatically and her serum calcium concentration was restored to normal. Two years following surgery, her serum PTH and Ca levels remain stable.
INTRODUCTION
Successful resection of mediastinal tumor is usually achieved with precise localization and estimation of the extension or invasive nature of the disease. Recently, video-assisted thoracoscopic surgery (VATS) is preferred to thoracotomy or sternotomy because it provides a magnified view with small skin incision and less pain.
Functioning adenoma is rare among mediastinal tumors. Due to its relatively small size and benign nature, surgeons often hesitate to operate. Therefore, accurate preoperative evaluation, histological confirmation during surgery and medical management for postsurgical complications are all essential for its successful treatment.
Here, we report a case of primary hyperparathyroidism due to a mediastinal parathyroid adenoma that was managed successfully by thoracoscopic resection. In this case, detailed preoperative information and magnified visual fields through thoracoscopy led to correct tumor identification during surgery, despite dense adhesions due to pleurisy. Thus, VATS resection should be the recommended treatment for functioning mediastinal parathyroid adenoma.
CASE REPORT
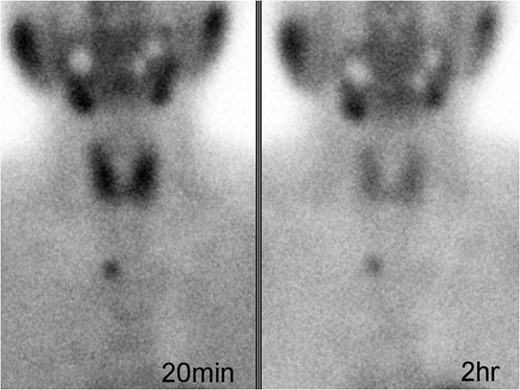
Technetium-99-sestamibi (99mTc-MIBI) imaging showing focal uptake during early (left) and delayed (right) phases in the mediastinum.
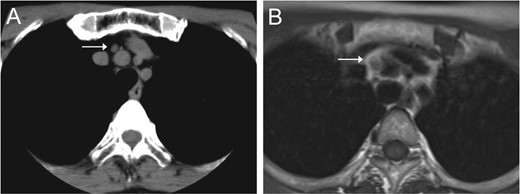
Chest CT (A) and MRI (B) revealed a mediastinal nodule adjoining the BCA.
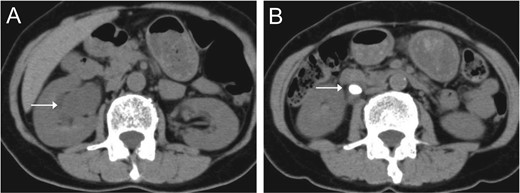
Abdominal CT indicated right hydronephrosis (A) and ureteral stones (B).
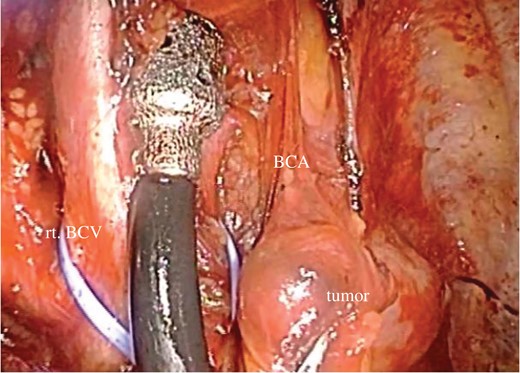
Thoracoscopic view of the mediastinal tumor.
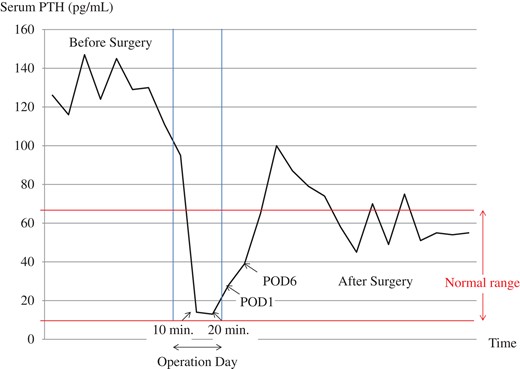
Serum PTH concentrations before and after surgery. After the immediate reduction during surgery, serum PTH level returned to normal range.
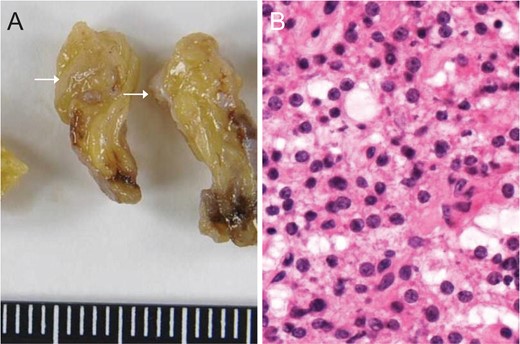
Macroscopic (A) and microscopic (B) views of the nodule confirmed the diagnosis of ectopic parathyroid adenoma.
The patient subsequently underwent extracorporeal shock wave lithotripsy for the remaining ureteral stones and was given monthly administrations of oral bisphosphonates. Her abdominal pain disappeared, and serum calcium/PTH levels have been stable 2 years following surgery.
DISCUSSION
Hormone-secreting parathyroid adenoma is a common cause of hypercalcemia. Combinations of symptoms classically described as ‘stones, bones, moans, groans and psychic overtones’ are rarely observed, whereas usual clinical manifestations are ureteral stones and bone mineral loss [1]. Persistent risk of intractable urolithiasis or osteoporosis and cost of medical intervention favor surgical removal of the tumor.
Primary parathyroidism usually results from excessive secretion of PTH from the cervical parathyroid gland. In contrast, ectopic parathyroid adenomas can be located in any part of their embryonic migratory path [2]. Among them, functional ectopic mediastinal parathyroid adenomas are relatively rare which account for 1–2% of patients undergoing surgical intervention [3].
The precise localization of adenoma is vital for accurate diagnosis. Imaging modality includes cervical ultrasound, CT, MRI and parathyroid scintigraphy. Whereas high-resolution sonography is a reliable method for localizing cervical parathyroid glands, 99mTc-MIBI scanning is the gold standard for initial discovery of ectopic adenomas. Other imaging techniques include positron emission topography CT/MRI and dual energy CT [4].
Management of hyperparathyroidism depends on clinical manifestations. Criteria for surgery in asymptomatic primary hyperparathyroidism suggested by the latest guidelines include: (i) serum calcium >1 mg/dl above upper limit of normal; (ii) markedly reduced bone density or presence of vertebral fracture on spine imaging; (iii) creatinine clearance <60 ml/min, presence of nephrolithiasis or nephrocalcinosis, or marked hypercalciuria (>400 mg/dl) and (iv) under 50 years of age. Patients need to meet only one of these criteria to be recommended for surgery [5].
In general, surgical approach for mediastinal tumor depends on its location and extension, including cervical approach, thoracotomy, and median sternotomy. Thoracoscopy provides magnified visual fields with small skin incision, which is especially useful for localization of small nodules [6, 7].
PTH monitoring during operation is valuable as serum PTH concentration declines immediately after tumor resection [8]. Intraoperative pathological confirmation is also helpful because surrounding fat/thymic tissue or mediastinal lymph nodes can make small adenomas indistinguishable. Although postoperative hypocalcemia is reported to be mild and asymptomatic, close follow-up of serum calcium levels is also important. Oral calcium tablets may be required to prevent severe hypocalcemia.
In conclusion, a case of hyperparathyroidism due to an ectopic PTH-secreting adenoma in the mediastinum was successfully treated by thoracoscopic tumor resection. 99mTc-MIBI scanning was useful in the initial detection of the adenoma. Intraoperative PTH level decreased immediately after tumor removal and has been stable thereafter. Precise localization, adequate preoperative evaluation, appropriate surgical approach and management of pre-/postoperative clinical manifestations are all essential for successful management of this disease.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}