





Abstract
Double pyramidal lobe is a scarce anatomical variation of the thyroid gland. Its presence impinges on the completeness of total and subtotal thyroidectomy and the postoperative treatment. Surgeons should be always aware of this variation in order to perform sufficient resection of the thyroid gland and minimize the possibility of recurrence of benign and malignant thyroidopathies.
INTRODUCTION
Double pyramidal lobe (DPL) of the thyroid gland is an extremely rare anatomical variation that has been reported only twice in the literature [1, 2]. The presence of this variation may encumber the completeness of total and subtotal thyroidectomy, which is usually the treatment of choice for benign and malignant diseases of the thyroid gland [3]. This is the first case of total thyroidectomy on a patient with DPL reported in Greece.
CASE REPORT
A 45-year-old female was operated for benign multinodular goiter. The patient had been receiving T4 per os as medication for 2 years according to the endocrinologist's instructions but the size of the nodules had been increased.
At the admission to our institution, the patient had had palpable, movable thyroid nodules, without hoarseness or palpable cervical lymph nodes. Blood tests, including T3, T4 and TSH had been in the normal spectrum. An ultrasound scan had revealed several tumescent nodules on the right and the left thyroid lobes. Following these, total thyroidectomy had been scheduled.
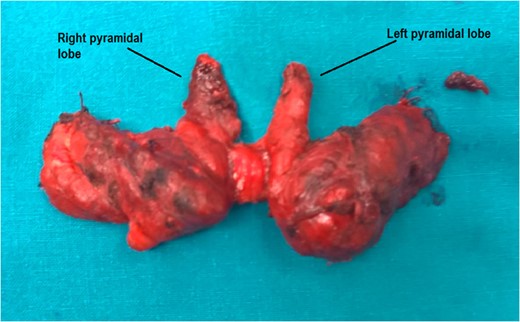
The DPLs of the thyroid gland.
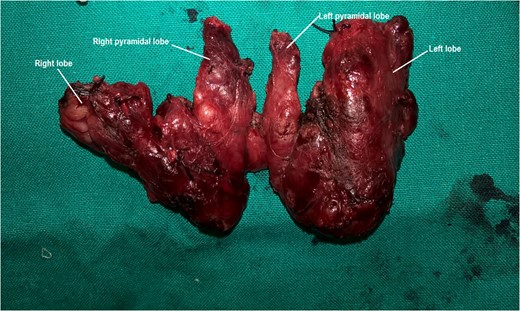
: Total resection of the thyroid gland. All the four lobes and the isthmus are detected. Nodules of the thyroid parenchyma are visible.

: A crude measurement of the thyroid gland size.
DISCUSSION
The pyramidal lobe may be considered as an anatomical anomaly, a morphological variation or a typical part of the thyroid gland [4]. The prevalence of its presence is 12–65% [5, 6]. As part of the thyroid gland, pyramidal lobe may originate from the right, the left lobe or the isthmus of the gland [3]. This lobe may be connected to the thyroid cartilage or it may be attached to the hyoid bone [4, 7]. Its length and size may vary, so that the pyramidal lobe can be characterized short (≤15 mm), medium (16–30 mm) or long (≥31 mm) [3]. Typically though its length is twice longer in females comparing to males [7]. Its form may be pyramidal, inverted Y, nodule or string [7]. In the presented case, DPLs were unexpectedly detected during total thyroidectomy. Only two other similar cases have been documented in the literature [1, 2].
Embryological studies suggest that pyramidal lobe represents the inferior part of thyroglossal duct [6]. Additionally, it is said that the presence of an extended lower part of the thyroglossal tissue leads to augmentation of the size of this lobe [4].
Although rare, the presence of DPL is of great clinical significance. In fact, the pyramidal lobes as parts of the thyroid parenchyma may be striked by diseases that affect the rest of the thyroid gland [4]. Diffuse thyroid diseases, such as multinodular goiter, Grave's disease or Hashimoto thyroiditis do more often affect the pyramidal lobe rather than focal thyroidopathies, such as thyroid tumors, due to its minor size in comparison to the rest of the gland [5].
Occurring to this, macroscopic, complete resection of the pyramidal lobes in total thyroidectomy, as in the present case, is compulsory, since any thyroid tissue remnant poses the possibility of recurrence of benign or malignant diseases of the thyroid gland [5, 7, 8]. Indeed, pyramidal thyroid tissue remnants can result in recurrence of benign multinodular goiter, years after the inadequate total thyroidectomy, developing as midline neck swelling [9]. Moreover, incomplete removal of pyramidal lobe may decrease the successfulness of postoperative radioactive iodine ablation, because the remnant lobe absorbs a large amount of the isotope [10]. When recurrence occurs, a reoperation poses a higher relative risk of complications comparing to an extended, meticulous primary total thyroidectomy [9]. In case of probable recurrence of malignant diseases due to pyramidal remnants, scintigraphic imaging, cervical computed tomography and FNA test are required to establish the diagnosis.
Thus, DPL should be carefully removed, as performed in the presented case, and the anterior cervical region should be promptly investigated intraoperatively for thyroid tissue remnants [4, 7]. Unfortunately, preoperative diagnosis of pyramidal lobes that could ameliorate surgical planning and technique is uncommon. Ultrasonography may be helpful, but preoperative scintigraphic imaging rarely detects its presence [5, 7].
In conclusion, DPL is a variation of key clinical significance since it affects the completeness of surgical treatment and the recurrence of benign and malignant thyroidopathies. Surgeons should be always aware of this anatomical anomaly and certify the performance of complete resection of both pyramidal lobes in hemithyroidectomy and total thyroidectomy in order to achieve better therapeutic outcomes.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}