





Abstract
Elasto fibroma dorsi is a rare tumour of the shoulder girdle that usually arises at the infra scapular area. We present a 57-year-old male with a soft tissue swelling on his right infra scapular area of 6 months duration. It was a painless lesion which caused him discomfort while sleeping. Preoperative imaging revealed bilateral tumours but the left tumour was impalpable. The surgery itself was uneventful but post-operatively he developed a haematoma which was managed conservatively Elasto fibroma is a benign pseudo tumour of the shoulder girdle. It’s aetiology is tied in to repetitive trauma of the shoulder girdle resulting in a pseudo tumour at the infra scapular area. Magnetic resonance imaging is the diagnostic modality of choice and is pathognomic in the presence of bilateral infra scapular tumours. Treatment is usually conservative and tissue diagnosis is essential as it can mimic a soft tissue sarcoma radiologically.
INTRODUCTION
Elasto fibroma Dorsi (ED) is a benign pseudo tumour of the shoulder girdle that commonly arises at the infra scapular area on the posterior rib cage. It is usually seen in females in the sixth decade of life and is bilateral in 30% of patients [1]. Male patients make up 10% of all cases and bilateral tumours in a male patient is extremely rare [1]. Magnetic resonance imaging (MRI) is the imaging modality of choice and surgery usually entails a simple excision due to a low risk of recurrence [2]. A tissue diagnosis is required to exclude a soft tissue sarcoma or if conservative management is being contemplated [3].
CASE REPORT
A male patient, 57 years of age was referred with a soft tissue swelling of 6 months duration. The lesion was palpable at the right infra scapular area on his back. He was referred to a surgeon due to its increase in size that caused him discomfort when laying down to sleep. There was no history of trauma and clinically he had no pain. There was no significant family history for soft tissue tumours.
Clinical examination revealed an indurated lesion at the right infra scapular area. There was no palpable thrill, bruit or clinical signs of sepsis. The mass was immobile. He had a normal range of movement at his right shoulder joint and his power, tone and reflexes were normal bilaterally. His upper limb neurological examination was unremarkable. He had no significant medical history. Ultrasound done at the referral hospital indicated a deep soft tissue swelling such as an elastofibroma or a sarcoma.
MRI confirmed the diagnosis and showed a second lesion on his left side, also at the infrascapular area (Figs 1–3). The patient had not complained of any symptoms to his left side or his left shoulder joint. After an extensive discussion with the patient and his family, we decided on a computerized tomography (CT) guided true cut biopsy to confirm the diagnosis (Fig. 4).
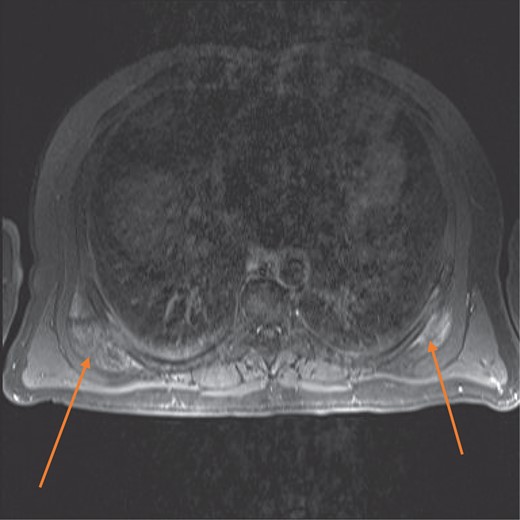
MRI axial view showing bilateral elasto fibromas (orange arrows) on the posterior rib cage.
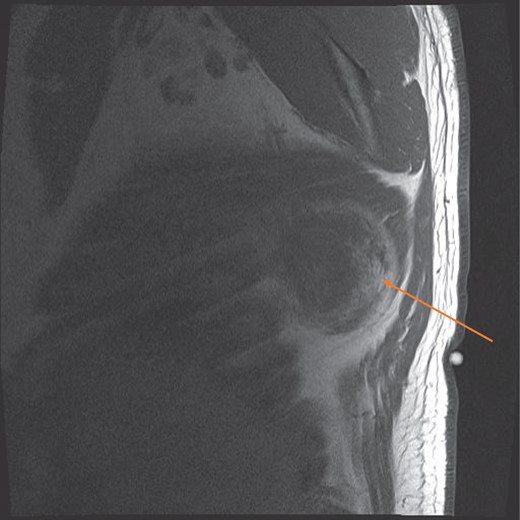
MRI sagittal view showing the circumscribed right sided tumour with a pseudocapsule, at the infrascapular region (orange arrow).
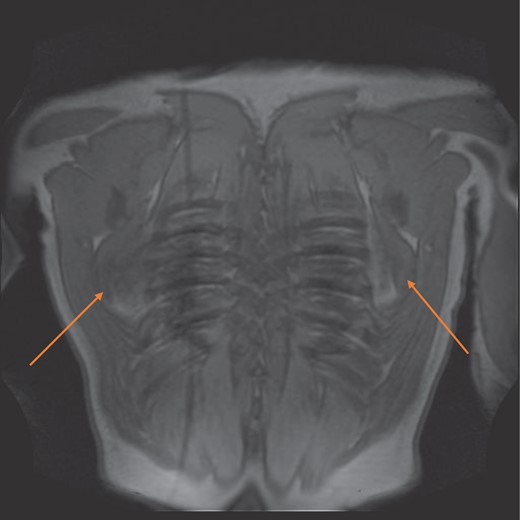
MRI coronal view of bilateral elastinfibromas (orange arrows).
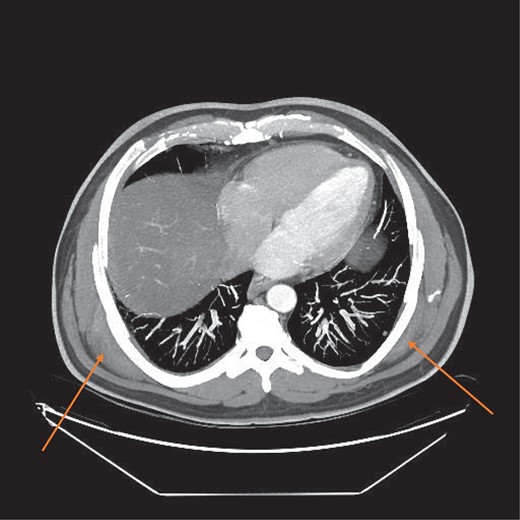
CT scan axial view showing bilateral tumours (orange arrows).
The tissue sample was inadequate for diagnosis and at this stage the patient decided to proceed with surgery in the form of an excision biopsy rather than a repeat CT guided biopsy. We decided to excise the symptomatic lesion on the right side first and then reevaluate the left side post-operatively. The left sided lesion remained asymptomatic and clinically impalpable.
Surgery was uneventful but the tumour was quite deep below the lattisimus dorsi and serratus anterior muscles, and lying on the posterior rib cage (Figs 5–7).
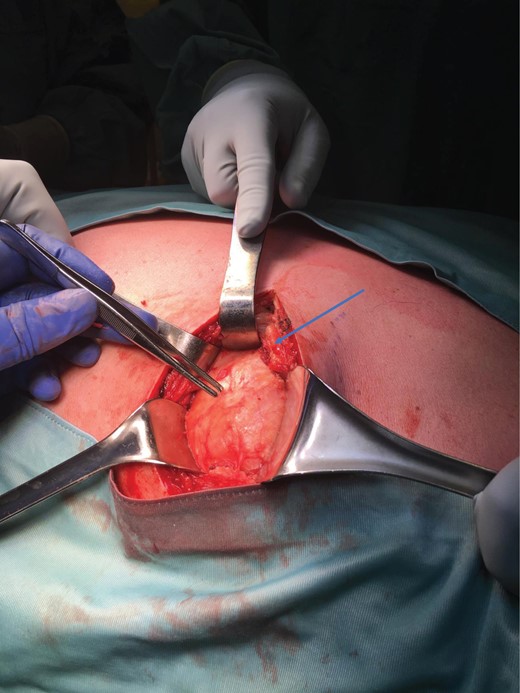
Tumour exposure(forceps) below the lattisimus dorsi (blue arrow).
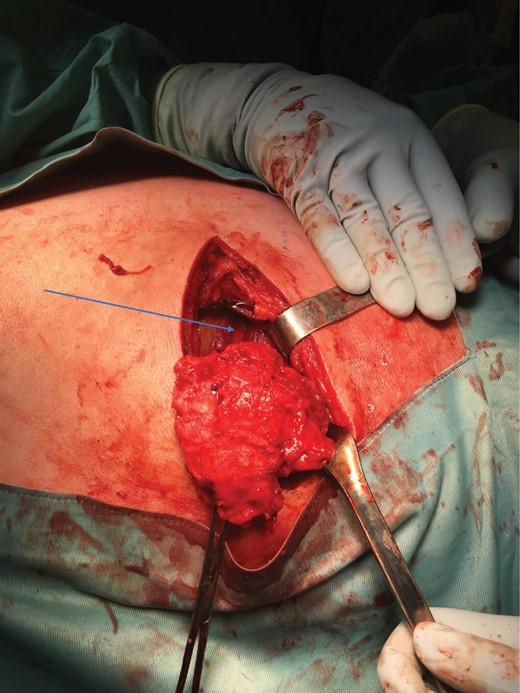
Tumour removed off the posterior rib cage (blue arrow).
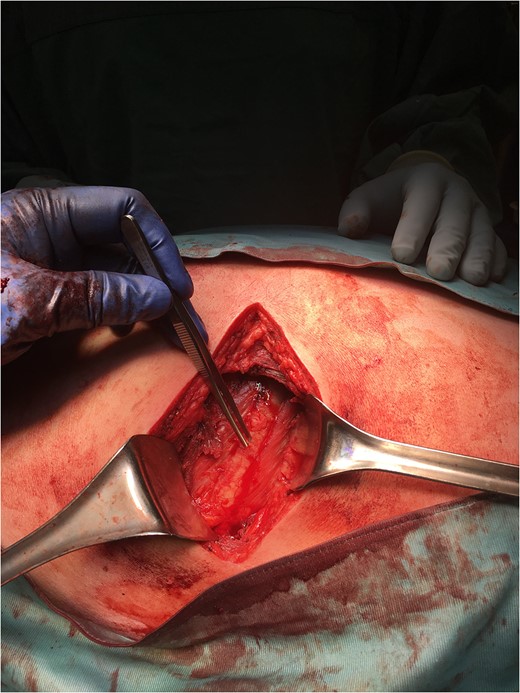
Posterior rib cage(forceps), post-tumour excision.
Post-operatively he developed a wound haematoma that was managed conservatively and eventually resolved (Figs 8 and 9).
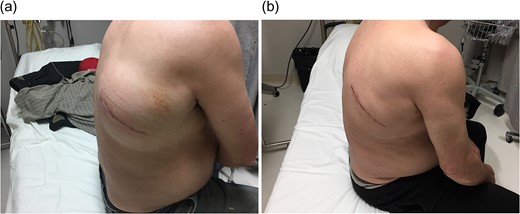
(a) Post-operative haematoma (b) Haematoma resolution with conservative management.
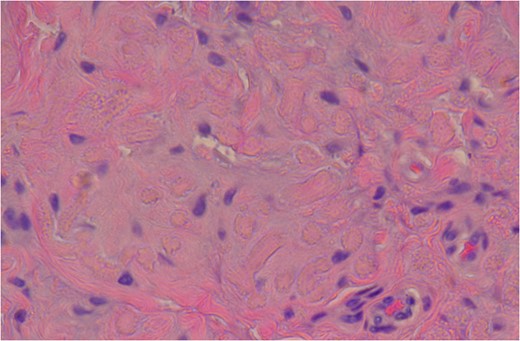
High Power slide showing elastic fibres (pink areas) which confirms the diagnosis of elastofibroma. (Altered elastic fibres in a collagenous matrix).
He did not develop any neurological sequelae such as an injury to the long thoracic nerve. This results in winging of the scapula, usually a rare complication of a level two axillary lymph node clearance in breast cancer surgery. Formal pathological results confirmed the diagnosis of an elastofibroma dorsi (Fig. 10).
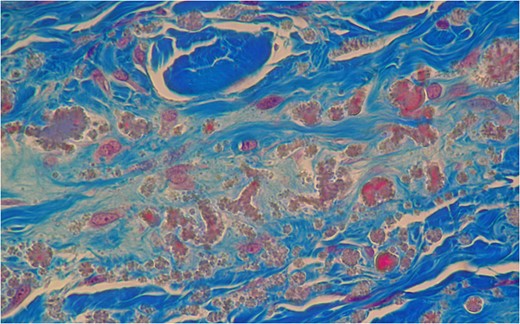
Mason’s Trichome stain outlining collagen around the abnormal elastic fibres with the characteristic serrated edges or petalloid globules. It outlines the elastic fibres by negative staining.
DISCUSSION
Elastofibromas are rare benign soft tissue tumours of the shoulder girdle and are more commonly seen in women than men. Brandser et al. reported an incidence of two percent in patients over 60 years of age on CT imaging with a female: male ratio of 11:1 [4]. The tumour is usually located at the infra-scapular area below the serratus anterior muscle on the posterior ribcage.
They are usually singular and bilateral tumours of the shoulder girdle are extremely rare and account for 10 percent of these tumours [5].
This adds to the uniqueness of this case report in that it is a male patient in his fifth decade of life with bilateral tumours. The tumours are usually asymptomatic and if the diagnosis has been confirmed histologically they can be managed conservatively.
The pathogenesis remains nebulous though there is some evidence that repetitive trauma results in degeneration of the collagen fibres and the formation of this pseudo tumour at the inferior pole of the scapula [6]. The fibro-elastic tissue at the inferior pole acts as a shock absorber that transmits force from the upper limb to the shoulder girdle [7].
A second theory involves a genetic predisposition as it can occur in patients with a positive family history as well. Surgery is only indicated for symptomatic patients or if there is a doubt about the diagnosis as these tumours can mimic a soft tissue sarcoma radiologically. Tissue diagnosis serves a dual purpose. It reassures the patient and clinician if they decide to continue with conservative management for asymptomatic tumours and secondly that a marginal resection would suffice as opposed to a larger resection for a sarcoma if surgery is contemplated [8].
Histological sections show an admixture of alternating collagen bundles with abnormal elastic fibres. The elastic fibres have a degenerate fragmented appearance of petalloid globules or chenille bodies. The Verhoeff stain confirms these abnormal elastic fibres [9] (Fig. 9).
The Mason’s Trichrome stain also confirmed the diagnosis by identifying the elastic fibres by negative staining. The elastic fibres appear brown on the histological slides [9] (Fig. 10). MRI remains the diagnostic imaging modality of choice. It has the added advantage of detecting contralateral subclinical lesions which would clinch the diagnosis as in this case. A second issue is the left sided tumour which was not excised at the original surgery. The patient continues to remain asymptomatic on the left side and the tumour remains clinically impalpable. The patient has opted for conservative management of this lesion in the interim. There has been no increase in size to date and we have decided on serial imaging unless the patient becomes symptomatic.
CONCLUSION
Elastofibromas are rare soft tissue tumours of the shoulder girdle and their need for a definite tissue diagnosis belies their ability to mimic a sarcoma radiologically. MRI allows for a presumptive diagnosis especially in the setting of bilateral tumours located infra scapularly. This case report is unique in that it is a male patient with bilateral tumours, which is extremely rare and accounts for 10% of all elastin fibromas. He is also a decade younger than the reported patient cohort.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}