





Abstract
Abdomino-scrotal hydrocele (ASH) is a very rare clinical entity. It is an unusual condition, in which there is an hourglass communication between a large hydrocele and the retroperitoneal space, through the inguinal canal. First described by Dupuytren in 1834 and defined by Bickle in 1919, the condition is rarely seen. Surgical management usually involves excision of the sac as the definitive treatment option. The pathogenesis of ASH remains unclear and numerous theories have been postulated. We favour the term scrotal-inguino-retroperitoneal (SIR) hydrocele as a more accurate description. The paper presents a unique case of a 24-year-old gentleman, with a functioning kidney transplant, who developed a large ASH/SIR hydrocele that required a midline laparotomy to fenestrate the sac.
INTRODUCTION
Abdomino-scrotal hydrocele (ASH) is a very rare clinical entity. It is an unusual condition, in which there is an hourglass communication between a large hydrocele and the retroperitoneal space, through the inguinal canal [1]. First described by Dupuytren in 1834 and defined by Bickle in 1919, the condition is rarely seen [1]. Surgical management usually involves excision of the sac as the definitive treatment option. We present a unique case of a 24-year-old gentleman, with a functioning kidney transplant, who developed a large ASH that required a midline laparotomy to fenestrate the sac.
CASE REPORT
A 24-year-old gentleman, with a kidney transplant, presented with a large right sided scrotal swelling. An MRI pelvis revealed a large right sided hydrocele with a clear communication between the scrotum and peritoneal cavity (Fig. 1). The gentleman was known to have an anterior syringocoele, which was diagnosed antenatally. He suffered with early postnatal renal failure, requiring haemodialysis. He consequently had an initial deceased donor kidney transplant aged 20 months, with the kidney placed in the right retroperitoneal space, and the anastomosis of the transplant renal artery and vein to the aorta and IVC, respectively. He had an open removal of this initial transplant due to recurrent urosepsis via a midline incision. He subsequently underwent a second living donor kidney transplant at 17 years of age.
An initial right inguinal approach was made. The retroperitoneal segment of the hydrocoele was identified and was densely adherent. Therefore, a laparotomy was performed via the previous midline incision to fenestrate the sac in to the peritoneum, as it was not safe to dissect the entire sac from the retroperitoneal structures. The vas deferens was especially at risk but together with cord was safely preserved. The cord was safely dissected from the sac and an inguinal hernia repair was performed using mesh. A right transverse scrotal incision was performed to undertake a Jaboulay eversion of the scrotal hydrocoele. The patient made a very good post-operative recovery and was discharged after 4 days.
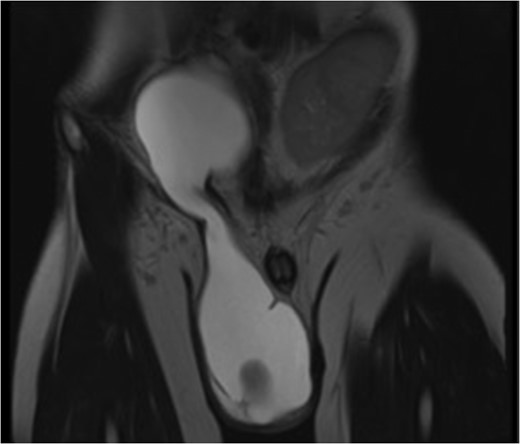
T2 weighted MRI pelvis (coronal section). MRI pelvis demonstrates a massive communicating ASH/SIR. A characteristic ‘hourglass’ shape is shown, along with the left sided transplant kidney
DISCUSSION
ASH was first described by Dupuytren as ‘hydrocele en bissac’ in 1834 [2]. Bickle defined the phenomenon as an ASH in 1919 [3]. ASH remains a rare entity, especially in adults. Awareness of the condition in the paediatric population is relatively higher. This is the first reported case of an ASH in a patient with a kidney transplant that we are aware of.
The pathogenesis of ASH remains unclear and numerous theories have been postulated. Dupuytren initially theorized that intracystic pressure exerted by an infantile hydrocele may push it through the deep inguinal ring and in to the abdomen [4]. It has also been proposed that as the radius of the fluid collection secreted by the tunica vaginalis increases, the inward pressure decreases, according to LaPlace’s law. This allows the collection to distend above the deep inguinal ring, and develop into the abdominal component of the hydrocele [2]. It has therefore been suggested that ASH be more accurately described as ‘scrotal-inguinoabdominal’ hydrocele [1], but we favour scrotal-inguino-retroperitoneal (SIR) hydrocele.
ASH, or SIR hydrocele, is generally a benign condition. Clinical diagnosis is based on bimanual palpation with the finding of two swellings, abdominal and inguino-scrotal, demonstrating pathognomonic cross fluctuation. Compression of the scrotal swelling may evacuate fluid into the abdominal swelling, and upon release will allow refilling of the scrotal component. This has been named ‘springing back ball’ sign [1]. Ultrasound is used to confirm the clinical findings, and may be useful to delineate other genitourinary pathology. CT or MRI can also be used to confirm initial suspicion, and to demonstrate the classic ASH hourglass shape, as seen in this report, through the inguinal canal.
Surgical correction of ASH/SIR hydrocele is the treatment of choice. A variety of surgical techniques have been described, amongst which the most common are inguinal, combined laparoscopic and inguinal, and scrotal approaches [4,5]. However, in our case, the initial inguinal approach was insufficient as the sac was densely adherent because of previous retroperitoneal surgery. It was also important to remain away from the bladder intraoperatively to minimize the risk of injury to the transplant ureter. A midline laparotomy was necessary to fenestrate the sac in to the peritoneum, and a Jaboulay eversion was undertaken for the scrotal hydrocele.
CONFLICT OF INTEREST STATEMENT
The authors declare that they have no conflicts of interest with the contents of this article.
REFERENCES
Author notes
Mr. R Srinivasan takes responsibility for the integrity of the content of the paper.

{kind=link}