





Abstract
Laparoscopic inguinal herniorraphy is a commonly performed procedure given the reported decrease in pain and earlier return to activity when compared with the open approach. Moreover, robotic assistance offers the operating surgeon considerable ergonomic advantages, making it an attractive alternative to conventional laparoscopic herniorraphy. Robotic herniorraphy utilizes the transabdominal preperitoneal approach where following repair peritoneal closure is necessary to avoid mesh exposure to the viscera. Self-anchoring sutures are frequently used to this end given the ease of use and knotless application. We present an unusual case of post-operative small bowel obstruction following robotic inguinal hernia repair caused by the self-anchoring suture used for peritoneal closure. This patient presented 3 days post-procedure with symptoms and cross-sectional imaging indicative of small bowel obstruction with a clear transition point. Underwent laparoscopic lysis of a single adhesive band originating from the loose intraperitoneal end of the suture leading to resolution of symptoms.
INTRODUCTION
Inguinal hernia repair is one of the most commonly performed surgical procedures with approximately 20 million inguinal herniorrhaphies’ repairs performed yearly around the globe [1]. The operative approach to inguinal herniorraphy overtime has evolved from primary tissue-based repairs to open tension-free mesh repairs and finally more recently laparoscopic mesh repairs. The latter has gained favor due to the substantial decrease in pain experienced by patients and an earlier return to activity [2]. Moreover, within the realm of laparoscopy, robotic assistance offers the operating surgeon considerable advantages in terms of superior visualization, stabilization of instruments and improved ergonomics, making this application an attractive alternative to conventional laparoscopic inguinal herniorraphy [3]. Robotic-assisted inguinal hernia repair utilizes the transabdominal preperitoneal approach (TAPP) which entails development of a peritoneal flap (PF), dissection and reduction of the hernia sac and placement of a mesh in the preperitoneal space thus created. Following hernia repair PF should be closed thereby partitioning the mesh from the viscera consequently reducing the risk of mesh erosion into the viscera and bowel obstruction secondary to herniation through the peritoneal defect [4]. There are many methods available for closure of the PF including sutures, tacks, adhesive sealants and staples; however, suture closure is preferred particularly in robotic TAPP as it allows complete exclusion of the preperitoneal space with an improved short-term quality of life [5]. In recent years, self-anchoring barbed sutures have been developed and gained popularity for a variety of tissue applications due to the simplicity of use and knotless application [6]. Herein we report an unusual case of post-operative small bowel obstruction following robotic-assisted inguinal hernia repair emanating from the self-anchoring suture used for PF closure.
CASE REPORT
A 61-year-old male with a weight of 88 kg and a BMI of 27 kg/m2 presented with symptomatic right-sided reducible inguinal hernia. He had no hernia-specific comorbidities or history of prior abdominal surgical procedures. He was offered and subsequently underwent a robotic-assisted TAPP inguinal herniorraphy. During the operation, a right-sided direct inguinal hernia was identified, the sac was completely reduced and hernia repaired with right-sided 15 × 10 cm Monofilament Polyethylene Terephthalate mesh (ProGrip™; CovidienTM Dublin Ireland). Following successful placement and fixation of the mesh PF was closed using 02-00 self-anchoring-barbed suture (V-Loc™ 180 Absorbable Wound Closure Device; CovidienTM Dublin Ireland). Total operative time was 124 min with 5 ml estimated blood loss and the patient was discharged home from post-anesthesia care unit.
The patient presented to the emergency department on post-operative Day 3 with complaints of nausea, vomiting, abdominal distention and obstipation. Physical examination revealed a tender and distended abdomen, further evaluation with cross-sectional imaging revealed a transition point in the right lower (Fig. 1). He subsequently underwent diagnostic laparoscopy where a free end of the barbed suture was noted to be adherent to the small bowel creating a sharp angulation in the bowel leading to obstructive symptoms (Fig. 2). The suture was lysed close to the peritoneum, which led to the relief of bowel obstruction. Post-operatively the patient had return of bowel function the following day and was discharged home.
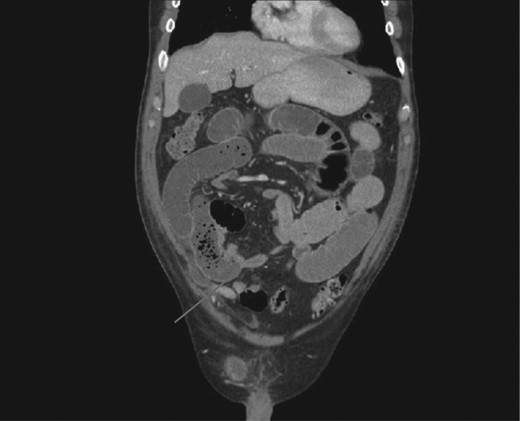
CT scan demonstrating transition point between dilated proximal and collapsed distal small bowel.
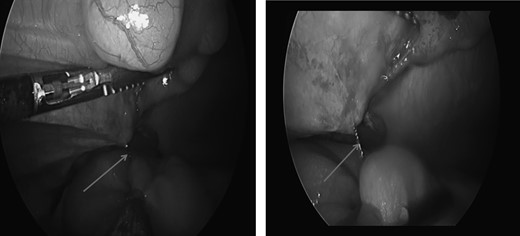
Laparoscopic view of self-anchoring suture adherent to the small bowel causing the obstruction.
DISCUSSION
Complete closure of the PF following a TAPP inguinal hernia repair is important to prevent post-operative complications. Available evidence suggests that closure of PF with running suture is preferable due to a reduction in post-operative pain [5] and incidence of bowel obstruction secondary to herniation through the peritoneal defect or displaced tacks [4, 7]. Self-anchoring knotless-barbed sutures offer an easier and faster option for PF closure. While these devices facilitate PF closure given their propensity of adherence to intra-abdominal viscera, there remains a risk of adhesive bowel obstruction. There have been some previous reports of small bowel obstruction following ventral rectopexy, sacral colpopexy and laparoscopic TAPP suggesting that if these devices are used maximal efforts should be made to ensure that the suture material is not exposed to any intra-abdominal viscera [8–10].
Conflict of interest statement
None declared.

{kind=link}
{kind=link}