





Abstract
We report a case of an intra-adenoma pituitary metastasis secondary to undiagnosed lung cancer. An 80-year-old man presented with rapid visual loss effecting his left eye secondary to a pituitary tumour. Following endoscopic transphenoidal resection, histology revealed that the pituitary tumour consisted of a metastatic lung adenocarcinoma contained within a pituitary adenoma. This case highlights a rare cause to be considered in the differential diagnosis of a patient presenting with abrupt visual loss.
Introduction
Sellar tumours are commonly encountered in neurosurgical practice and a clear understanding of the differential diagnoses is essential when assessing such patients. We present a case of metastatic disease occurring within a pituitary adenoma. Metastases are rare causes of pituitary tumours, however, do form part of the differential. However, a metastasis with a known adenoma is very rare indeed. Furthermore, this case illustrates the clinical features, which may differentiate an intra-adenoma metastasis from other pathologies such as a recurrent pituitary adenoma or metastatic disease within a normal pituitary gland.
Case Report
An 80-year-old man presented with rapid onset visual loss predominantly affecting his left eye. He presented 5 years prior to this with a progressive deterioration in vision associated with a pituitary tumour and at that time underwent endoscopic transphenoidal surgery; however, an incomplete resection was achieved. The original histology confirmed the tumour to be a benign pituitary adenoma. Post-operatively, his vision improved initially and he was managed by the endocrinology team for hypopituitarism. At follow-up, visual field testing and MR scanning showed that the residual tumour was clinically and radiologically stable. His pituitary ademona was considered stable for 5 years until he re-presented.
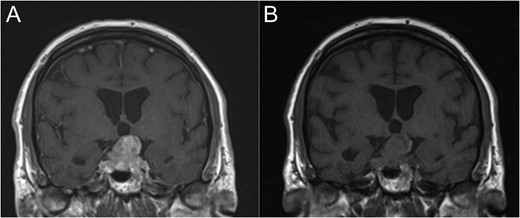
Coronal T1-weighted MRI with (A) and without (B) Gadolinium contrast enhancement.
By far the most likely diagnosis at representation would be a recurrence of the original adenoma. If malignancy elsewhere was known, then a metastasis may have been considered. Given this was a de novo presentation of metastatic lung carcinoma, the diagnosis was something of a surprise.
Revision endoscopic pituitary surgery was carried out and intra-operatively the tumour was noted to be very firm and vascular. Approximately 400 ml of blood was lost intra-operatively, compared to 150 ml during the original surgery. The patient did not experience any post-operative complications.
The immunohistochemistry revealed that the pituitary tumour consisted of a metastatic lung adenocarcinoma contained within a pituitary adenoma. This lead to a diagnosis of lung cancer, which was previously unknown. The patient was subsequently managed under the Oncology team and treated with chemotherapy. Unfortunately, the patient's vision continued to deteriorate and it was felt that he would not be a suitable candidate for further surgery.
Discussion
Pituitary tumours are frequently seen in neurosurgical practice and pituitary adenomas are the most common type in adults. Pituitary adenomas are the third most common intracranial tumour and have a prevalence of approximately 76–94 per 100 000 population. Recurrence following endoscopic transphenoidal resection has been described, and the risk has shown to be greater in patients with post-operative residual tumour. Furthermore, the median time to recurrence is ~5 years.
In our case, the patient presented 5 years following an incomplete resection; therefore, a recurrence of his pituitary adenoma was seen as the most likely cause of his symptoms.
Metastatic involvement of normal pituitary gland is rare and is associated with a poor prognosis. The most frequently found primaries are breast and lung cancer. Pituitary gland metastases are symptomatic in only 7% of patients, in such patients, diabetes insipidus is the most common presenting feature. There are no specific radiological features of pituitary metastases, which distinguish them from benign pituitary adenomas. Nevertheless, concurrent cerebral metastases should raise suspicion of malignant pituitary pathology. We report a case of a solitary intracranial mass lesion located within the sella turcica occurring in the absence of diabetes insipidus or a past medical history of systemic cancer. Therefore, metastatic disease was not initially considered in the differential diagnosis.
Metastatic disease involving a pituitary adenoma is rare and few cases have been reported [1–3]. The presenting features differ to that of metastases occurring within normal pituitary gland, they are more likely to present with visual as a posed to diabetes insipidus. Moreover, the visual loss is likely to be rapid [2, 3], when compared with the gradual deterioration seen in benign pituitary adenomas. These differentiating clinical features are highlighted in our case; his initial visual loss was slow and progressive, correlating with the growth of a benign adenoma, whereas his second presentation consisted of a rapid deterioration in vision, which represented intra-adenoma metastatic pathology.
Pituitary adenomas are a potential site for metastatic spread of systemic cancers. Intra-adenoma pituitary metastases may occur in patients with a known cancer or may be the presenting feature of previously undiagnosed cancer. A rapid onset of symptoms may indicate a more malignant tumour as the underlying cause.
Conflict of interest statement
None declared.

{kind=link}