





Abstract
An emergency thoracotomy may be life-saving by achieving four goals: (i) releasing cardiac tamponade, (ii) controlling haemorrhage, (iii) allowing access for internal cardiac massage and (iv) clamping the descending aorta to isolate circulation to the upper torso in damage control surgery. We theorize that a new goal should be achieving rapid, large-volume fluid resuscitation and we describe a technique to achieve this.
INTRODUCTION
With penetrating trauma reaching epidemic proportions in the Caribbean [1], emergency room (ER) thoracotomies are performed regularly [2]. It may be life-saving by achieving four goals: (i) releasing cardiac tamponade, (ii) controlling haemorrhage, (iii) allowing access for internal cardiac massage and (iv) clamping the descending aorta to isolate circulation to the upper torso in damage control surgery [3, 4]. We theorize that a new goal should be achieving rapid, large-volume fluid resuscitation and we describe a technique to achieve this.
TECHNIQUE
An important step during ER thoracotomy is to detect cardiac tamponade by opening the pericardium with a vertical incision that avoids the phrenic nerve. The heart is now exposed, providing the perfect opportunity for catheterization.
In this technique, we place a large, curved Satinsky clamp across the base of the right atrial appendage. Sharp scissors are used to make a 5-mm incision in the atrial appendage. Bleeding is minimal once the Satinsky clamp effectively isolates the appendage. A 20Fr Foley's catheter is then inserted into the incision, ensuring that the balloon is fully within the atrial appendage. The balloon is not inflated because there is insufficient space with the clamp applied. A heavy suture with a round-bodied needle is used to place a purse string around the incision. The suture is tied firmly to achieve a water right seal around the catheter.
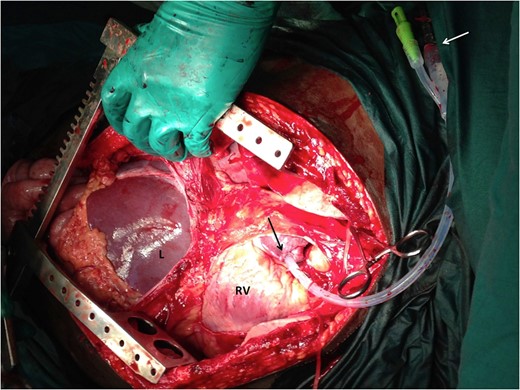
Photograph during an ER thoracotomy. The pericardium has been opened to reveal the right ventricle (RV) and atrium. A Foley's catheter has been introduced into the right atrial appendage (black arrow) and fixated with a purse-string suture. A white arrow demonstrates the fluid administration set connected to Foley's catheter.
DISCUSSION
Intravenous access is difficult to establish in these volume-depleted patients since there is peripheral vasoconstriction. This technique allows rapid intravenous access because intra-cardiac catheterization can be achieved in 1–2 minutes with the heart already exposed at ER thoracotomy. Furthermore, the volume of fluid that can be infused exceeds that which can be delivered by peripheral large bore cannulae.
The procedure is easy to perform and requires little specialized equipment. Even in the resource poor setting, a Foley's catheter and suture material are readily available. Application of the Satinsky clamp sequesters blood within the right atrial appendage but it does not interfere with venous return or right atrial outflow tracts. Therefore, there is no interruption of cardiac output while this is performed.
Closure is simple and effective. We have used the technique routinely in our ER thoracotomies with good effect [5]. It allows large-volume fluid infusion to proceed, while the surgeon searches for sources of continued haemorrhage.
CONCLUSION
Four life-saving goals can be achieved at ER thoracotomy: (i) tamponade release, (ii) haemorrhage control, (iii) internal cardiac massage and (iv) clamping of the descending aorta. Rapid, large-volume resuscitation should be the fifth goal at ER thoracotomy. This technique is easily performed and requires little specialized equipment. It allows better resuscitation that may contribute to increased survival rates.
ACKNOWLEDGEMENTS
None.
Conflict of Interest Statement
None declared.
Funding
None.
REFERENCES
Author notes
All authors contributed equally to this work

{kind=link}