





Abstract
We present a case on abdominal wall abscess from spilled stones post-cholecystectomy and describe laparoscopic drainage as our choice of management. Mr M is a 75-year-old male who presented on multiple occasions to the hospital with right upper quadrant pain and fever post-laparoscopic cholecystectomy. He also required multiple courses of antibiotics. Subsequent computed tomography and magnetic resonance imaging scan confirmed a number of retained stone with signs of chronic inflammation. Hence, 6 months after his initial laparoscopic cholecystectomy, he proceeded to an exploratory laparoscopy. We found an abscess cavity measuring 3 × 4 cm over the anterior abdominal wall. The cavity was de-roofed, drained and washed out. The tissue culture grew Klebsiella pneumoniae. Laparoscopic approach is optimal as the abscess cavity can be clearly identified, stones visualized and removed under direct vision. Patient does not require a laparotomy.
INTRODUCTION
With an increasing number of laparoscopic cholecystectomy performed, studies have reported gallbladder perforation of up to 40% of cases [1]. Complications may arise from these spilled stones postoperatively.
We present our case and describe laparoscopic drainage as our choice of management for chronic abscess caused by these spilled stones.
CASE REPORT
Mr M is a 75-year-old male who required repeated admission for right upper quadrant pain post-laparoscopic cholecystectomy.
During his initial operation, a chronically inflamed gallbladder was encountered. Multiple small gallstones in the gallbladder were present with iatrogenic perforation and spillage of stones. An Endo-bag was used to remove the gallbladder. A further washout was performed. Final histology confirmed chronic cholecystitis. He was discharged the day after with 1 week of oral antibiotics.
He presented 6 weeks later complaining of right upper quadrant pain and fever. He had a raised white cells count of 15 and an elevated C-reactive protein (CRP) of 110. A computer tomography (CT) abdomen (Fig. 1) was performed, which showed numerous calcific densities that were surrounded by soft tissue thickening and stranding. These were likely spilled stones. There was no evidence of collection. He was admitted for 2 days on Intravenous (IV) antibiotics then discharged.

CT showing the spilled stones.
He represented 2 months later with similar pain. He proceeded to an endoscopic retrograde cholangiopancreatography with normal cholangiogram. He then represented again 2 weeks later with ongoing pain and a raised white cells count of 16 and CRP of 48. A repeat CT was performed, which found a number of retained calculi, now lying at the postero–inferior aspect of the liver with signs of chronic inflammation. He was admitted for 5 days of IV antibiotics.
On discharge, he required regular visits to his general practitioner for antibiotics. He was seen at the clinic as a follow-up for his ongoing right upper quadrant pain. A magnetic resonance imaging (MRI) abdomen (Fig. 2) was performed, which showed small, oval-shaped, thick wall collection anterior to the capsule of the liver. After the MRI, we have decided to book him for surgery.
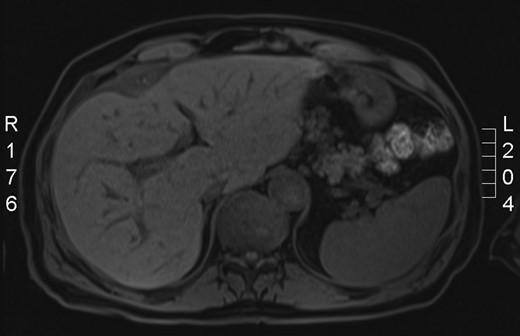
MRI showing the spilled stones.
Therefore, 6 months after his initial laparoscopic cholecystectomy, he proceeded to an exploratory laparoscopy. We found an abscess cavity measuring 3 × 4 cm over the anterior abdominal wall (Fig. 3). The cavity contained a lot of slough and pus. The cavity was de-roofed, drained and washed out. The tissue culture grew Klebsiella pneumoniae, sensitive to Augmentin. He was discharged the day after with 1 week of oral antibiotics.
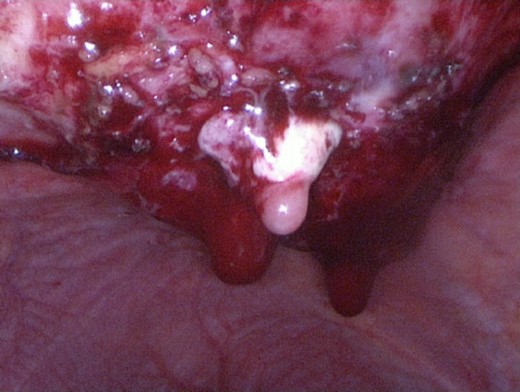
Laparoscopic view of the chronic abscess.
DISCUSSION
Complications caused by stone spillage post-cholecystectomy are rare with a rate of 1.7 complications per 1000 cases [2]. Zehetner reviewed all reported complications from stone spillage and found that abdominal wall abscess and intra-abdominal abscesses were the most common complications [3].
Our patient presented multiple times with abdominal pain secondary to an abscess from spilled stones. Other potential stone-related complications include adhesions, fistula, obstruction, intestinal perforation and pleural empyema [1].
Management of an abscess due to spilled gallstones includes draining the abscess and intravenous antibiotics. Furthermore, removal of spilled gallstones is important to prevent recurrence. Radiological and open drainage have been described. However, retrieval of stones can be difficult with radiological methods.
Mr M went to theatre for an exploratory laparoscopy. Using the Hasson technique, a 10 mm umbilical port was inserted to establish pneumo-peritoneum. Another 10 mm epigastric port and 5 mm right upper quadrant port were inserted. The abscess cavity was visualized and de-roofed with diathermy. This was sent for microbiology. Stones were also retrieved.
Laparoscopic approach is optimal as the abscess cavity can be clearly identified, stones visualized and removed under direct vision. Patient does not require a laparotomy.
Prevention is better than cure. Every attempt should be made to avoid spillage of gallstones during the initial surgery including careful dissection and identification of the correct planes. Extra care taken at this stage of the operation can save many minutes attempting to retrieve spilled stones later.
If spillage occurred, it should be recorded clearly in the operative notes. The surgeon should attempt to remove all visible stones at the time of surgery and use copious irrigation. There is no indication for routine conversion to open surgery to retrieve spilled stones.
It is also advisable that we should include this complication on our list of differential diagnoses when an unusual abdominal wall or cavity abscess develops in a post-cholecystectomy patient. If sizeable stones are seen on CT during the initial presentation, it should have been dealt with fairly early as the symptomatic stones are highly unlikely to resolve on its own. Management with laparoscopic drainage and retrieval of stones is feasible for some of these patients.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}