





Abstract
Ureteroduodenal fistula is a rare complication in urology. We report a case of 29-year-old man who presented with ureteroduodenal fistula. We have also discussed the management and treatment of this condition.
INTRODUCTION
Ureteroenteric fistulae are extremely rare entities. To our knowledge, only about a dozen cases have been reported in the literature in the past century. Most of these cases are ureteroduodenal fistulae and are usually associated with chronic or recurrent urinary tract infections. We encountered a patient with this condition. We would also like to review the literature on this rare condition.
CASE REPORT
We present a case of 29-year-old male who presented to the Department of Urology, Ratna Hospital, Pune with symptoms of burning micturition on and off for the past 4 months. The patient had a past history of right open ureterolithotomy and insertion of JJ stent for upper ureteric calculus around 8 months back. However, he did not follow up for stent removal for 8 months. During the present admission, patient's physical examination was unremarkable except for previous surgical scar. Urine routine showed 50–70 pus cells/hpf and had normal renal function. X-ray kidney ureter bladder showed a retained JJ stent in the right ureter with thick encrustations involving upper and lower ends of the stent. Ultrasound showed right-sided hydronephrotic kidney and the presence of encrustations, as shown on the X-ray.
The patient was initially subjected to lithotripsy (extracorporeal shock wave lithotripsy) for the encrustations over the stent and later taken up for removal of the retained stent. During this procedure, right ureterorenoscopy was performed to fragment thick encrustations present around the stent. However, upper end of stent was not visualized, and the attempt of stent removal had to be abandoned. On table right, retrograde pyelography (RGP) was performed. This showed contrast entering right pelvicalyceal system along with free flow of contrast outside the ureter into what looked like a part of small bowel (Fig. 1). Guide wire could not be negotiated into the kidney.

RGP finding.
At a later date (1 week later), he underwent exploration in view of ureteroenteric fistula. During surgery, we found a fistulous tract connecting the upper portion of the ureter with the third part of duodenum around 3 cm distal to the pelvis, with upper coil of JJ stent lying into the duodenum (Fig. 2). Fistulous tract was excised, and retained portion of the stent was removed. Duodenum was closed in two layers, and ureterotomy was closed over a new JJ stent. Patient tolerated the procedure well, and the JJ stent was later removed after 2 weeks.
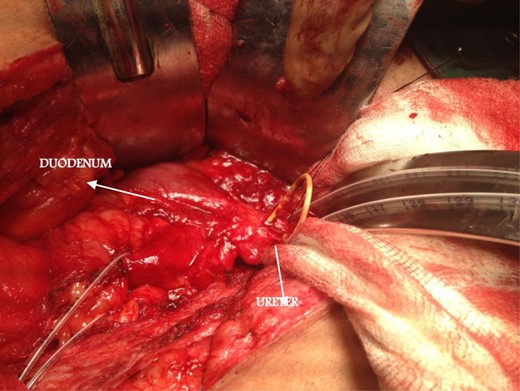
Intraoperative finding.
DISCUSSION
Ureteroduodenal fistulae are known but unusual complications. The first case was reported in 1918 by David, E.G. [1]. They have been reported to occur secondary to chronic renal infection, ureteric calculi, duodenal ulcer diseases, roundworm infestation of urinary tract, iatrogenic injury, trauma or ingestion of foreign body [2,3]. Patients usually present with recurrent urinary tract infections, flank pain, hematuria and diarrhea. The case we have reported is iatrogenic and followed surgery for stone disease. Management depends on the renal function. With normal renal function, ureteroureterostomy, excision of fistulous tract and reconstructive repair of the bowel are performed. If ipsilateral renal function is poor, nephrectomy may be required [2–4].
Ureteroduodenal fistulae are potentially dangerous complications of ureterolithotomy, particularly in situation where there is dense inflammation around the impacted stone. It should also be born in mind in all cases of difficult endoscopic maneuvers such as ureteroscopy for retained stent. Retained stents may form a source of intractable sepsis as well as technical difficulties in the management.
CONFLICT OF INTEREST STATEMENT
None declared.
ACKNOWLEDGEMENTS
The authors would like to thank the Department of Urology, Ratna Hospital, Pune, India.

{kind=link}
{kind=link}