





Abstract
Chylous ascites is a rare clinical entity that historically has been accompanied by high mortality due to the association with malignancy. Here we present a case of chylous ascites as a complication of mild pancreatitis in a young woman. We review the literature of similar cases, which revealed four similar cases with a range of outcomes. Treatment options vary from dietary restriction of medium chain fatty acids, total parental nutrition, radiological intervention and surgery.
INTRODUCTION
Chylous ascites is a rare clinical entity most commonly seen after major gastrointestinal surgery such as oesophagectomy, gastrectomy or pancreaticoduodenectomy. We present a case of chylous ascites discovered during a laparoscopic cholecystectomy in a young woman following an episode of mild pancreatitis.
CASE REPORT
A 39-year-old female, with a history of anxiety, presented to our metropolitan hospital with a 3-day history of central abdominal pain radiating through to her back with nausea and vomiting.
Initial laboratory investigations revealed serum lipase of 640 U/l (a normal range of 8–57), bilirubin 9 µmol/l (<25), ALP 160 U/l (30–120), GGT 132 U/l (<51), AST 36 U/l (<41) and ALT 39 U/l (<41). Abdominal ultrasound demonstrated gallstones and a diagnosis of biliary pancreatitis was made. After 7 days her pain improved and was discharged home.
A planned elective laparoscopic cholecystectomy was performed 3 days after discharge. Cholecystectomy was uncomplicated and an intra-operative cholangiogram was unremarkable. After resection and delivery of the gallbladder, there was an ongoing accumulation of milky fluid within the hepatorenal space. The fluid appeared chylous and a midline laparotomy was performed with an aim to identify the leak site. At the base of the mesentery small blocked lymphatics could be seen (Fig. 1). No definite site of chyle leakage could be identified. Two drains were placed, one in the gallbladder bed and other in the base of the mesentery. Analysis of the fluid demonstrated a chyle leak with triglyceride level of 410 mg/dl and amylase of 60. Serum triglycerides were 130 mg/dl.
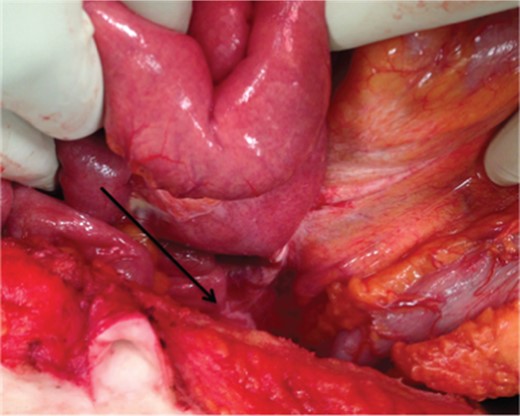
Intra-operative photo: dilated lymphatics at the base of mesentery (arrow).
Post-operatively, the patient was kept nil-by-mouth and given total parenteral nutrition. The patient was put on low fat diet 4 days later. The drains were removed on Day 15 post-operatively. The patient was well when seen again 6 months later.
DISCUSSION
Chylous ascites or chyloperitoneum is defined as a collection of chyle within the peritoneal cavity. Chyle is the only body fluid with a fat content greater than the plasma; therefore, chylous ascites may be diagnosed when the ascitic fluid triglyceride level is >110 mg/dl (1.25 mmol/l) [1]. The fluid is classically milk coloured, odourless and separates into a serous and fat layer.
Chylous ascites is a rare complication of pancreatitis. Only seven other case reports whereby pancreatitis was the cause of chyle leak were found in the English-based literature [2–8]. More commonly, it is associated with major abdominal operations, such as aortic aneurysm repair, pancreaticoduodenectomy or retroperitoneal lymphadenectomy [8]. Traditionally associated with a very high mortality of up to 71%, chylous ascites outside the operative setting is mostly related to intestinal and haematological malignancies [1].
Of the seven case reports, four reported on chylous ascites being discovered after or during cholecystectomy after an episode of biliary pancreatitis [3–5, 7]. Three of the four cases were mild episodes of pancreatitis, all undergoing cholecystectomy within 5–8 days as in this case [4, 5, 7]. The remaining one case identified the chylous ascites intra-operatively [7].
The presumed pathogenesis is disruption of abdominal lymphatic channels, thus it is most commonly seen after retroperitoneal surgical procedures. In the non-operative setting, such as pancreatitis, there must be disruption or obstruction to both the lymphatico-venous and lympho-lymphatic channels in order for sufficient lymphatic hypertension to occur such that peritoneal extravasation can occur.
Pancreatitis without cholecystectomy is a rare but recognized non-operative cause as well [2, 6, 8]. The two presumed mechanisms of pancreatitis-related chylous ascites are compression of lymphatics from an inflamed pancreas or direct damage of channels by pancreatic enzymes [3, 4, 8, 7].
As with most fistulas, the key to resolution is the reduction of the pressure causing the leak. There are many methods available for the management of a chyle leak. Non-operative techniques include fasting patients, feeding patients with medium-chain triglycerides (MCT) based diet or use of diuretics and somatostatin analogues. Dietary manipulation such as fasting patient or feeding with MCT diet reduces intestinal lymph flow. As such leak site would be allowed to heal spontaneously. This was shown to be very effective in our case above. The use of somatostatin analogues and diuretics is common; however, the efficacy of these medications is not well understood [9].
Invasive techniques involving interventional radiology or surgery tend to be used as second-line therapies. Lymphangiography using lipiodol as contrast agent has been shown to stop chylous leaks [9]. Surgical options such as exploration to ligate leaky lymphatic vessels or placement of a peritoneovenous (PV) shunt are considered last resort therapies. PV shunt unfortunately over the years has gained a notorious reputation in causing complications such as sepsis, disseminated intravascular coagulopathy and even mortality [1].
In conclusion, chylous ascites from gallstone-related pancreatitis is an uncommon clinical entity. The exact mechanism related to its pathogenesis is not fully understood, although two main theories exist. As exemplified by this case, chyle leak post-pancreatitis can be managed successfully with conservative measures incorporating an MCT diet or parenteral nutrition.
CONFLICT OF INTEREST
None declared.

{kind=link}
{kind=link}