





Abstract
Endometriosis is a common gynecologic disorder wherein ectopic endometrial glands and stroma are found at extrauterine sites. Extrapelvic endometriosis is a well-documented, yet rare, disease entity that can affect almost any organ system. Inguinal endometriosis is an extremely rare disease entity characterized by tender inguinal swelling. Here we report a case of a sudden-onset and acutely painful left inguinal hernia with concordant endometriosis. A review of the literature is presented. The presence of isolated endometriosis contained within a left-sided inguinal hernia sac has, to our knowledge, never been reported. Often diagnosed incidentally or on histologic examination, general surgeons should consider inguinal endometriosis in the differential diagnosis of inguinal masses, even in the absence of catamenial symptoms. Surgical excision, with gynecologic follow-up, is locally curative and the treatment of choice for inguinal endometriosis.
CASE REPORT
A 23-year-old healthy female was admitted to our hospital with a new-onset tender bulge in her left groin, associated with subjective fevers and chills. Four days prior to presentation, she noted a sudden protrusion in her left groin with associated pain. Given worsening pain and intermittent nausea, she presented to our emergency room. On admission, physical examination revealed a soft, non-distended abdomen that was tender to palpation in the left lower quadrant. A soft, mobile, exquisitely tender, and non-reducible mass was appreciated in her left groin, concerning for an inguinal hernia. She had an unremarkable medical and gynecologic history and no prior surgical history. Laboratory data were notable for a leukocyte count of 6.7, a hematocrit of 36.9 and a lactate of 1.4 in the setting of normal electrolytes. An outside ultrasound showed an avascular complex cystic lesion measuring 2.1 cm in the left groin. A subsequent computed tomography scan of the abdomen and pelvis revealed a tubular cystic structure along the left inguinal canal, coursing along the expected path of the round ligament, without surrounding fat stranding or herniation of bowel loops. Given her symptoms and the unclear etiology of the hernia, she was admitted to the hospital and taken to the operating room for exploration (Fig. 1). In the operating room, a 6-cm dark purple cystic structure was visualized within the sac of an indirect inguinal hernia, travelling along the round ligament down toward the mons pubis (Fig. 2). The cystic structure was dissected away from the round ligament and the cyst was opened and noted to contain clear liquid. Ultimately, the patient underwent left indirect inguinal hernia repair, with Gore Bio A absorbable mesh, and excision of a left inguinal hydrocele of the round ligament. Final pathology revealed fibromuscular tissue lined by mesothelium consistent with a hernia sac and a hydrocele with concordant endometriosis. The patient's post-operative course was uneventful and she was discharged home on post-operative Day 1.
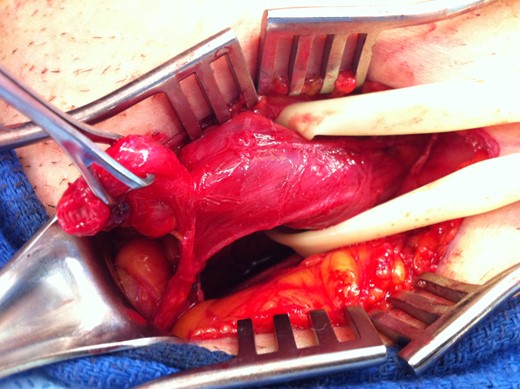
Left indirect inguinal hernia.
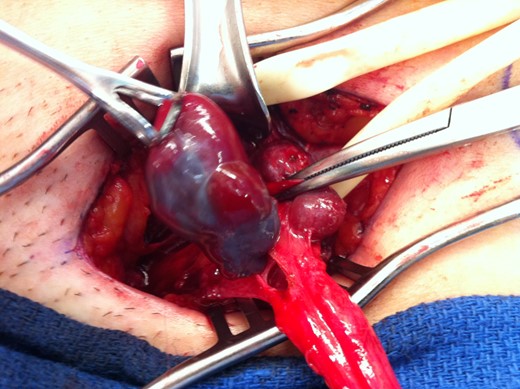
Purple cystic structure within the sac of an indirect inguinal hernia, travelling along the round ligament down towards the mons pubis.
DISCUSSION
Endometriosis is defined as the presence of ectopic endometrial glands and stroma at extrauterine sites. It is a relatively common, benign, estrogen-dependent disorder that affects ∼10% of women of reproductive age. It is characterized by chronic pain, severe dysmenorrhea and infertility, although the disease may be asymptomatic or discovered incidentally. Endometriosis can affect almost any organ system, although most ectopic implants are located in the pelvis. Extrapelvic endometriosis is a rare disease entity that may cause a variety of unusual symptoms, including pain and physiologic dysfunction, dependent on the location and size of lesions as well as the organ system affected. It has been described at multiple sites including the gastrointestinal tract, urinary tract, thoracic cavity, central nervous system, umbilicus, skin (including abdominal wall incisions and episiotomy scars) and inguinal canal.
Inguinal endometriosis is a condition characterized by the presence of endometrial stroma and glands in the extraperitoneal portion of the round ligament and in the surrounding connective and lymphatic tissues. First described in 1986, it is an extremely rare affliction with <60 cases reported in the literature. The best available estimates suggest that it may affect 0.3–0.6% of patients with endometriosis [1]. Typically, patients are in their reproductive years, with a peak incidence between 30–40 years, and present with tender inguinal swelling [2]. Inguinal endometriosis is difficult to recognize and thus often confused with more common conditions such as hernias, lymphadenopathy, granulomas, soft tissue tumors, cysts and hydroceles. Catamenial symptoms, such as variation in size and tenderness of the mass, are present in 50% of cases and should raise the index of suspicion for inguinal endometriosis [3]. In many cases, the patient is brought to the operating room with a preoperative diagnosis of incarcerated hernia and the endometriosis is discovered incidentally or on histologic examination.
In over 90% of cases, inguinal endometriosis occurs on the right side [4]. The endometriosis most often affects the extraperitoneal portion of the round ligament and is rarely found in association with occult hernias. However, in a minority of cases, inguinal endometriosis can coincide with inguinal hernias and other groin pathology, increasing the diagnostic difficulty. In one series, 37% of patients suffered from inguinal endometriosis associated with a groin hernia [3]. The presence of isolated endometriosis contained within a left-sided inguinal hernia sac has, to our knowledge, never been reported. In all but two cases reported in the literature, or 91% of cases, concordant pelvic intraperitoneal endometriosis has been identified [3].
The treatment of choice for both inguinal hernias and inguinal endometriosis is surgical excision. In order to be locally curative, surgical excision must include the removal of the extraperitoneal portion of the round ligament. Complete excision of the lesion prevents recurrence and allows for histological diagnosis. Given the high concordance of pelvic endometriosis, concurrent diagnostic laparoscopy or post-operative referral to a gynecologist is indicated to evaluate for other lesions and the extent of endometriosis. In some cases, there may be a role for hormonal suppression with oral contraceptives or GnRH agonists. Our patient underwent complete excision of a left inguinal hydrocele of the round ligament and repair of left indirect inguinal hernia with mesh. She was started on hormonal therapy with an oral contraceptive and subsequently referred to a gynecologist for subsequent evaluation of her newly documented endometriosis.
AUTHORS’ CONTRIBUTIONS
K.A., C.G., S.O. and A.G. all contributed to the writing of this case report. All authors were members of the clinical team who saw the patient and treated the patient at the Beth Israel Deaconess Medical Center. The case report was written in large part by K.A. with contributions from all other authors.
FUNDING
No financial support to acknowledge.
CONFLICT OF INTEREST
No conflict of interest to disclose.

{kind=link}
{kind=link}
{kind=link}
{kind=link}