





Abstract
Radical resection of primary or solitary secondary malignant sternal tumours is indicated in patients without metastases. Sternal reconstruction may be indicated in large defects to prevent pulmonary complications, to achieve protection of intra-thoracic organs and to obtain a good aesthetic result. In this article, a modified surgical technique is described to fill and reconstruct large defects after radical resection of a primary or secondary malignant sternal tumour. The technique makes use of a methyl methacrylate composite within two layers of polypropylene mesh enforced by steel wires through the sternal ends of the defect enhancing stability. This modified technique can be easily applied, making curative broad radical resections of the sternum feasible.
INTRODUCTION
Primary malignant tumours of the sternum are rare, mostly chondrosarcomatous lesions, while loco regional recurrences of breast cancer more frequently present as secondary tumours. Patients often have a history of tumour recurrence treated with surgery, systemic chemotherapy and radiotherapy. Surgical resection of these lesions especially improves quality of life and survival [1, 2] when radical resection is performed and surgical margins have been shown to be free of tumour cells. As a consequence, radical resections may lead to large sternal and costal surgical defects. As such defects pose a reconstructive challenge, many surgeons are reluctant to perform such a procedure. However, from a clinical point of view, reconstruction of the sternum is paramount in preventing pulmonary complications as flail chest and paradoxical breathing [3] and in providing adequate protection of intra-thoracic organs [4].
While various techniques have been proposed to treat and provide adequate coverage of sternal defects [3, 5, 6], these techniques offer little stability. To address this issue, we present a modified technique possibly offering greater stability through the use of sternal cerclages through the sternal ends of the defect.
CASE REPORT
A 60-year-old male patient presented himself to the outpatient clinic of our department with a progressive sternal mass. An MRI scan indicated a tumour involving the manubrium extending to the first and second ribs and involving the right clavicle and sternoclavicular joint (Figs 1 and 2). Based on radiological evaluation, a core biopsy was obtained and a low-grade chondrosarcoma was characterized. Radiological evaluation indicated primary tumour resection to be the treatment of choice. Radical excision of the tumour was performed and resulted in resection of the manubrium, as well as the medial third of the right clavicle and the right first and second ribs. Steel wires through the sternum and left sternoclavicular joint spanned the 6.5 cm sternal defect (Figs 3 and 4) and a polypropylene mesh filled with methyl methacrylate composite (Surgical Simplex®), Howmedica Osteonics, Limerick, Ireland, was placed, yielding a stable reconstruction of the sternal defect (Figs 5–8). The sternocleidomatoideus muscle was re-inserted to the polypropylene mesh. Pathological examination showed complete excision of the tumour. The patient recovered uneventfully and was discharged 7 days post-operatively. At seven year follow-up, the patient displayed excellent functional and aesthetic results. Optimal function of his shoulders allowed a complete return to work and other activities without disabilities.
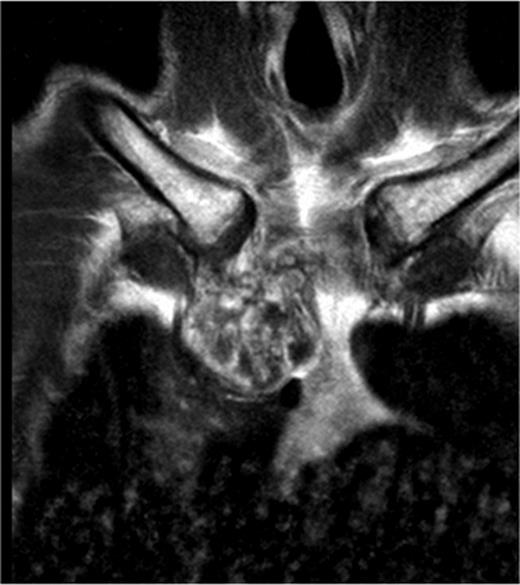
A MRI scan of a patient showing a tumour involving the manubrium extended to the first and second ribs including the right clavicle and sternoclavicular joint.
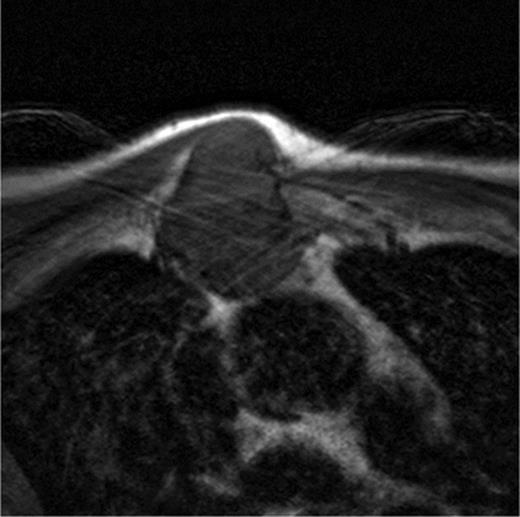
The axillar slides of the MRI of the patient showing the ingrowth of the tumour in the thoracic cavity in relation to the intrathoracic organs.
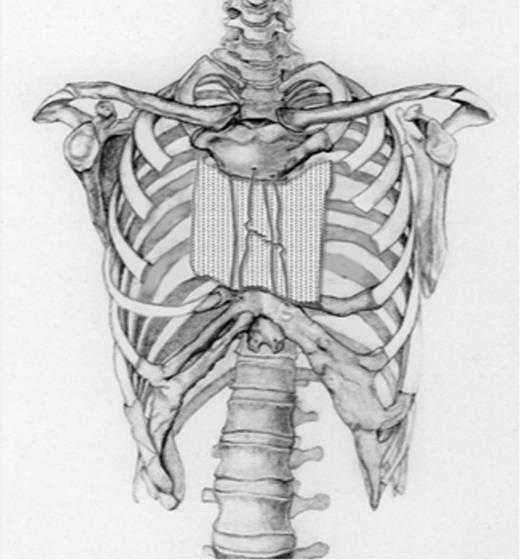
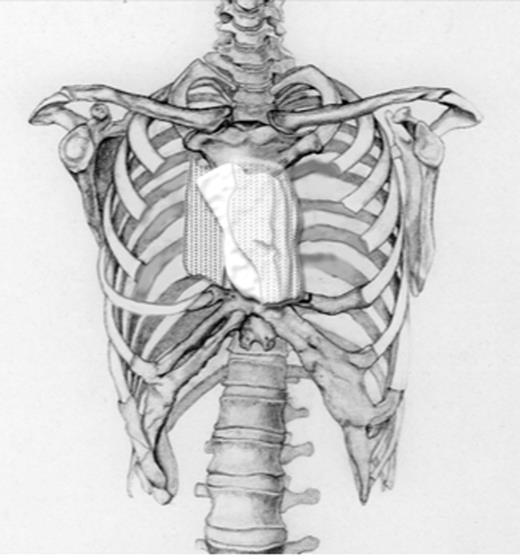
Schematic drawing of the size of the defect after radical excision followed by placing steel wires through the stenal ends.
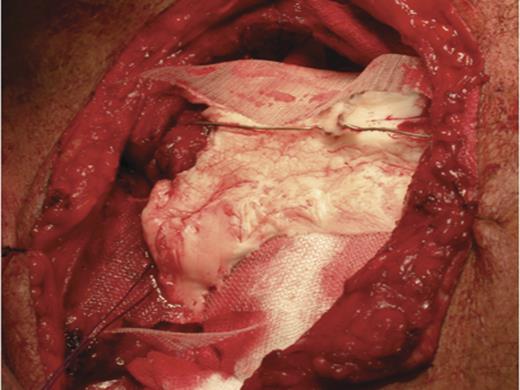
This picture shows the size of the defect in the patient after radical resection, which was 6.5 centimetres. Consequently, steel wires were placed through the sternal ends and the left sternoclavicular joint and a polypropylene mesh was place on the surface of the defect.
Schematic drawing showing a polypropylene mesh filled with methyl methacrylate composite to reconstruct the sternal defect.
Around these steel wires a polypropylene mesh was placed filled with methyl methacrylate composite to reconstruct the sternal defect.
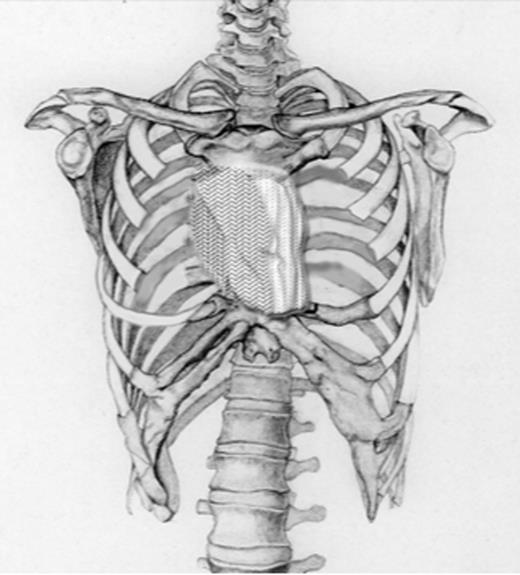
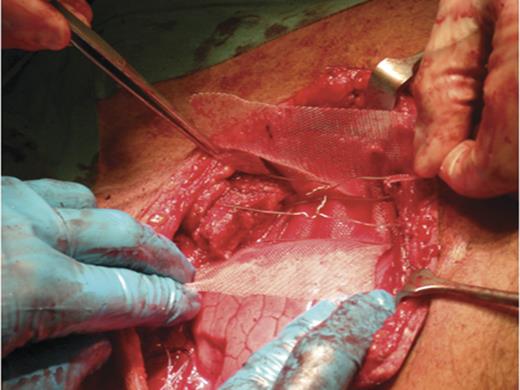
Schematic drawing showing the final reconstruct after tumour resection of the sternum.

This picture shows the final reconstruct after tumour resection of the sternum in the patient.
DISCUSSION
Radical resection of primary or solitary secondary malignant sternal tumours is indicated in patients without metastases. Adequate reconstruction of the sternum after tumour resection by use of a stable construction prevents pulmonary complications like flail chest or paradoxical breathing, while protecting underlying structures and offering good functional and aesthetic results [5]. Creating a stable reconstruction of the sternum can be challenging, leaving many surgeons reluctant to perform thoracic wall resections including parts of the sternum. Previous studies describe a Marlex Mesh reconstruction, primarily focusing on covering the sternal defect and optionally applying a methyl metha-acrylate composite [6, 7]. The choice of the type of reconstruction usually depends on the surgeon's preference. The use of methyl methacrylate and polypropylene mesh as a sandwich [5] is most often employed in an attempt to generate a stable construction. However, there is no evidence that this technique offers full stability of the sternum.
In this article, we describe a relatively simple and modified technique to provide a functionally stable construction of the sternum after (sub) total resections of malignant sternal tumours. Additionally, by recreating the natural shape of the sternum, the technique provides optimal aesthetic and functional results.
Four types of sternal defects are usually defined; (1) partial longitudinal sternectomy with resection of less than 75% of the sternal width, (2) subtotal lower sternectomy, (3) subtotal upper sternectomy and (4) subtotal mid sternectomy.
Patients undergoing a partial longitudinal sternectomy of maximally 50% of the sternal width do not necessarily require a rigid reconstruction, regardless of the part of the sternum involved. Novoa et al. describe low morbidity and a shortened postoperative recovery phase through the use of the Sandwich method in patients requiring such resections combined with involvement of two or more ribs [8]. Generally, a full reconstruction is only indicated with removal of tumours spanning the entire width of the sternum. Novoa et al. used muscle flaps alone or muscle flap in combination with the double polypropylene mesh and methyl methacrylate composite for reconstruction. In our opinion, this technique does not generate the required rigidity/stability of the reconstruction. We believe the use of steel wires connecting the cranial and caudal ends of the sternum provides the rigidity and stability needed, while possibly reducing pulmonary complications.
That the double polypropylene mesh and methyl methacrylate composite in these defects does not provide enough stability is confirmed by previous studies reporting the results of this technique in patients after subtotal mid, upper or total sternectomy. Weyant et al. [6] described 49 patients (34 partial sternectomy, 9 resection of the manubrium and 6 total sternectomy) with a 56% pulmonary complication rate. Of these patients, 8 patients had respiratory failure, 12 had pneumonia, 8 had atelectase-requiring bronchoscopy and one had aspiration. Recently, novel rigid fixation techniques are introduced using titanium bars and clips or the titanium fixation system using plates and screws with excellent functional results [9, 10].
In conclusion, our modified technique using polypropylene mesh containing methyl methacrylate composite enforced with steel wires seems to be simple and reliable, while making curative broad radical resections feasible. Additional research is required to describe the outcomes of this new technique in a larger patient population.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}