





Abstract
Neostigmine is an acetylcholinesterase inhibitor that is increasingly used as a medical treatment in cases of pseudo-obstruction. It has a well-recognized side-effect profile that includes bradycardia and bronchospasm. We present a case of colonic perforation after administration of neostigmine in the treatment of pseudo-obstruction.
INTRODUCTION
We report a case of colonic perforation following the administration of neostigmine for the treatment of pseudo-obstruction. Neostigmine is a prokinetic agent that is increasingly being used in the treatment of pseudo-obstruction. There is limited evidence of its efficacy and due to its side-effect profile it should be used with caution.
CASE REPORT
The patient, a 34-year-old female, developed symptoms consistent with pseudo-obstruction on Day 3 post-emergency Caesarean section, which was performed for foetal distress and possible placenta abruption. An abdominal X-ray was performed which showed a significantly dilated colon (Fig. 1), and the diagnosis of pseudo-obstruction was again confirmed on computer tomography (CT) scan of the abdomen which showed a caecum measuring 9.8 cm transversely (Fig. 2). Emergency colonoscopic decompression with the insertion of a flatus tube was performed and medical management, including cessation of opioids, anticholinergics and correction of electrolyte abnormalities, was commenced.
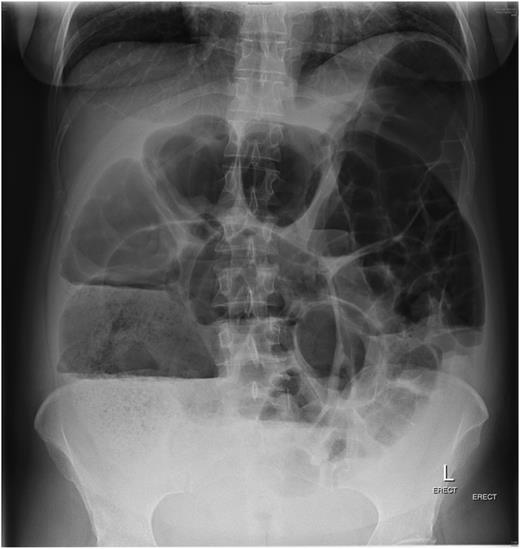
Plain abdominal X-ray consistent with pseudo-obstruction.
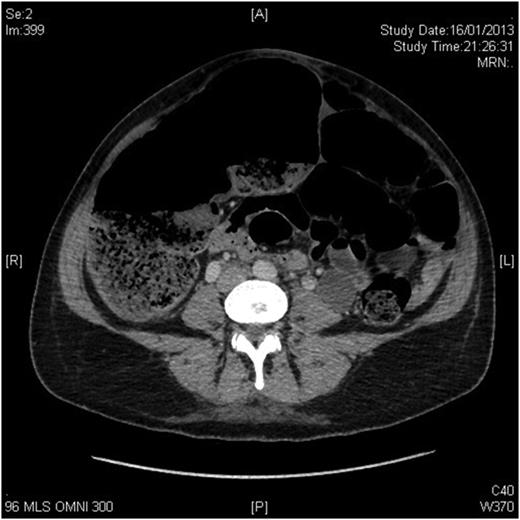
CT scan of the abdomen showing caecum measuring 9.8 cm transversely.
The patient failed to have a return of normal bowel function post-decompression and after 3 days was administered 500 µg of neostigmine via subcutaneous injection in an attempt to improve bowel motility. That evening she developed fever, and abdominal pain and erect chest X-ray confirmed free gas under her diaphragms (Fig. 3). She was taken to theatre for emergency laparotomy. At operation she was found to have two sites of caecal perforation with a moderate faecal contamination in the right paracolic gutter. A right hemicolectomy with primary anastomosis was performed. She was discharged home on post-operative Day 7 without further complication. It is possible that the serosal tears of the caecum had occurred secondary to either administration of neostigmine or dilatation in the post-Caesarean period.
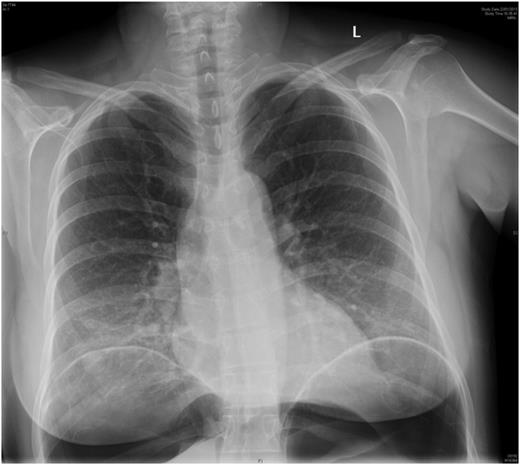
Erect chest X-ray confirming perforated visus.
DISCUSSION
Neostigmine is an agent that inhibits the effects of acetylcholinesterase thereby acting as a prokinetic. The first use of it in the treatment of pseudo-obstruction is attributed to Hutchinson and Griffiths in 1992 [1].Subsequently, there have been several small studies that report it as a safe and effective treatment in pseudo-obstruction [2–4]. It has several well-documented side effects including bradycardia, hypotension, headache, dizziness, muscle cramps, bronchospasm and salivation. There are however only two other reported cases in the literature of colonic perforation in association with the use of neostigmine for the treatment of colonic pseudo-obstruction [5, 6].
Patients with pseudo-obstruction are often unwell with up to 95% of cases associated with significant infection, trauma or recent surgery [7]. Whilst the documented risk of colonic perforation is low, being reported at ∼3%, these patients have a high risk of mortality due to these co-existing factors [8]. The use of neostigmine is not without risk due to its well-documented side-effect profile. Further work is required to examine whether the risk of perforation is increased in patients with pseudo-obstruction who are treated with neostigmine.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}