





Abstract
We report a case of a previously healthy woman after an uneventful caesarean section who developed polymicrobial necrotizing fasciitis. She was given a non-steroidal anti-inflamatory drug (NSAID) after her delivery. Her post-delivery course was complicated by septic shock, and required multiple debridements before abdominal reconstruction. This case describes the increased risk of necrotizing fasciitis with NSAID use. Unusual were the organisms causing the polymicrobial necrotizing fasciitis: Staphylococcus aureus, Enterobacter agglomerans, Acinetobacter baumannii, and two strains of Enterobacter cloacae.
INTRODUCTION
Necrotizing fasciitis remains a rare disease with an estimated 500 to 1000 cases annually in the United States (1). The majority of cases occur after minor trauma, and very rarely described after a variety of surgical procedures (2). Here we report a rare case of polymicrobial necrotizing fasciitis after a cesarean section.
CASE REPORT
A 24 year old at 38 weeks gestation (G3P2) presented to another hospital in labor. She had no past medical history, and previously had two previous caesarean sections. A 3.5 kg child was delivered by c-section under spinal anesthesia. She had an uneventful hospital course and was discharged uneventfully with Ibuprofen for analgesia.
The patient presented to our institution on the seventh post delivery day with abdominal pain, nausea, vomiting, and fever. Her vital signs included a temperature of 38.3° C, a heart rate with sinus tachycardia of 154/min, and a blood pressure of 85/47 mmHg. On physical exam she had a firm, diffusely tender abdomen, with guarding and rebound. There was mild erythema with a foul smelling, watery discharge from the incision. The wound was partially opened and probed, but there was no evidence of any collection or dehiscence. Her other admission laboratory tests were unremarkable except for a lactate of 3.5 mmol/L (normal: 0.5 – 1.0 mmol/L), a white blood cell count of 12.5K/mm3, and a prealbumin of < 2.7 mg/dL (normal: 16 – 35 mg/dL), indicative of severe protein calorie malnutrition.
In septic shock, including hypotension, acute lung injury, and oligura, the patient was intubated, required multiple pressors despite fluid resuscitation. Broad spectrum antibiotic coverage, including Meropenem, Vancomycin, and Doxycycline were initiated on admission. CT of the abdomen and pelvis were nondiagnostic; blood and urine cultures were negative. The patient continued to require increasing doses of pressors, remained oliguric, and remained in shock by her persistent lactic acidosis.
An exploratory laparotomy was performed, and an abscess was found in the rectus muscle at the base of the previous incision. The infection had tracked up through the rectus sheath bilaterally, with associated myonecrosis, and complete separation of the muscle from the anterior and posterior rectus sheath fascia. The reproductive organs were not involved in the abscess; the rest of the exploration was negative, except for edematous small bowel. The operative diagnosis was necrotizing fasciitis, and a wide debridement was performed. Intraoperative cultures revealed a polymicrobial infection, namely, Staphylococcus aureus, Enterobacter agglomerans, Acinetobacter baumannii, and two strains of Enterobacter cloacae. Because of the overwhelming infection and anticipated need for further debridement, the decision was made to manage the patient with a temporary abdominal closure utilizing the AbVAC (KCI). Pathology later confirmed the diagnosis of acute necrotizing fasciitis and myositis.
Post surgical debridement, the patient’s pressor requirement and renal dysfunction improved dramatically. The patient remained with an open abdomen for 28 days, with additional serial debridements, and twice weekly AbVAC changes (Fig. 1). The patient underwent an abdominal wall reconstruction using the component separation technique that was reinforced with biologic mesh and made a full recovery.
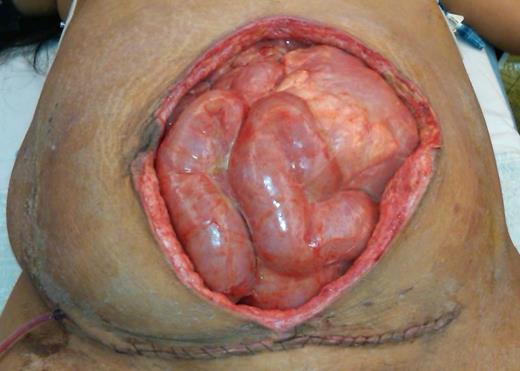
Open abdomen technique was used to facilitate the multiple operations. Note the loss of a portion of the anterior abdominal wall from the serial debridements.
DISCUSSION
Necrotizing fasciitis is a fulminant infection involving extensive areas of soft tissue necrosis, most commonly involving the limbs, perineum and abdominal wall (3). As in our case, a minor penetrating injury or a surgical incision is usually involved, with postoperative cases accounting for approximately 20% of the total (4). While Group A Streptococcus is the most common monomicrobial isolate, polymicrobial infections with a variety of gram positive, gram negative, aerobic and anaerobic isolates can also occur. The polymicrobial combination of our patient’s organisms is unique from previously described cases.
The aetiology of necrotizing fasciitis is not fully understood. Major risk factors include diabetes mellitus, as well as age greater than 50 years and appear to be associated with a higher mortality and morbidity (5). These factors were absent in our case, however necrotizing fasciitis following c-section has been reported following the administration of NSAIDs in the immediate post operative period (6). NSAIDs have been linked to necrotizing fasciitis in a temporal fashion. It is controversial if the NSAID effect is to simply mask the signs and symptoms, to delay diagnosis of the necrotizing fasciitis (7), or if inhibition of granulocyte chemotaxis, phagocytosis, and bactericidal activity, and depression of lymphocyte transformation documented to occur in vivo is occurring in these patients (8).
Most patients present with signs of inflammation such as erythema, swelling, and pain at the infected site. Severe pain disproportionate to local findings and associated with systemic toxicity should definitely raise the suspicion of necrotizing fasciitis. Radiologic plain film imaging reveals gas in the muscles and superficial fat in only approximately 35% of cases. CT scan may help distinguish cellulitis from necrotizing fasciitis and may help guide management (9). However, as in our case, a normal CT scan does not exclude the disease. Despite a patient’s unstable condition, surgical debridement should proceed, and not be delayed. It is important to note that serial debridement may be necessary and that closure of the fascia after the first debridement is not advisable to facilitate further operations. Leaving the abdomen open in this case is consistent with damage control laparotomy techniques, as well as prevention of abdominal compartment syndrome. Serial debridements may also limit the size of the final defect needing to be reconstructed.
Necrotizing fasciitis in the postpartum patient remains a rare challenge, with a high mortality. This patient’s rapid deterioration with septic shock and multisystem organ failure could have resulted in maternal death. Clinical suspicion must remain high, despite the rarity of the disorder, as early diagnosis is critical, and is most commonly made without confirmatory radiological imaging. Early aggressive debridement, of any and all necrotic tissue, forms the cornerstone of therapy, with additional serial debridements offering the best chance of survival.

{kind=link}