





Abstract
Internal iliac artery aneurysms are rare, but with a mortality approaching 50% in those that rupture, prompt diagnosis is essential. Often presentation is nonspecific; a wide variety of symptoms and signs have been encountered, illustrating a challenge in identification. We report a case of ruptured internal iliac artery aneurysm presenting as urinary retention. The importance of maintaining a broad differential in cases of urinary retention is clearly highlighted.
INTRODUCTION
Isolated internal iliac artery aneurysms are very rare, accounting for around 0.4% of abdominal aneurismal disease (1). With a rupture rate of 38% and associated high mortality, early detection and intervention is essential. Signs and symptoms at presentation are often nonspecific so a high index of clinical suspicion is required. Timely intervention in cases of isolated internal iliac artery aneurysm has the potential to improve survival.
CASE REPORT
An 84 year old, retired electrician, presented to the emergency department with reduced urine output and lower abdominal pain. He reported a three day history of urinary hesitancy and increased frequency, associated with generalised lower abdominal pain radiating to the testes. His medical history included transurethral resection of the prostate in 2005, inguinal hernia repair and hypertension. The patient lived alone and was an ex-smoker.
On examination he appeared well, with stable observations. He was noted to have lower abdominal tenderness, without being peritonitic, and had a palpable bladder. His testes were normal in appearance and non tender. A digital rectal exam was unremarkable. Urinary catheterisation revealed a residual volume of 300ml. A provisional working diagnosis of urinary retention was therefore made, with no cause identified.
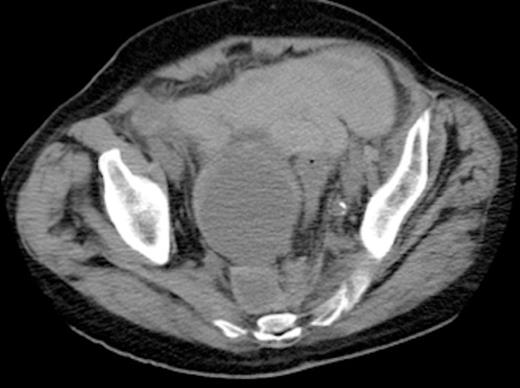
Axial view of CT abdomen-pelvis showing right internal iliac artery aneurysm with a contained pre-sacral leak (as indicated by arrow)
The patient deteriorated the following day, becoming hypotensive and anuric, with an increasingly tender abdomen. Haemoglobin levels dropped substantially and he developed a lactic acidosis. After initial resuscitation, an urgent CT scan of the chest, abdomen and pelvis showed an 8.5cm aneurysm of the right internal iliac artery. There appeared to be a contained leak from the aneurysm in the pre-sacral region (Fig. 1). A moderate amount of intraperitoneal free fluid was noted. A right sided hydronephrosis with associated right hydroureter was also noted.
An urgent transfer to a vascular facility was arranged and a same day endovascular repair of the aneurysm was performed.
DISCUSSION
Acute urinary retention is a common presentation in the emergency setting. Irrespective of aetiology, initial management usually involves bladder decompression – typically by catheterisation. Prompt identification of the underlying cause is then essential in directing further management. In elderly men causative factors can be grouped into: obstructive, neurogenic and detrusor inactivity. Benign prostatic hyperplasia is the most common individual cause but often there are multiple underlying factors (2). Careful history and examination, combined with the use of specific diagnostic testing will usually establish a cause, and therefore result in the identification of high risk patients (3).
Iliac artery aneurysms account for an estimated 2% of intra-abdominal aneurysmal disease, with a quarter of these primarily affecting the internal iliac artery. 10-20% of cases are associated with abdominal aortic aneurysm (4). Typically presentation is late, with an estimated 40% rupturing and a mortality of over 50% in those cases.
Identifying patients with internal iliac artery aneurysms of any size is challenging, because they often remain asymptomatic. In fact, incidental finding on imaging is the most common method of diagnosis. Patients may present with non specific symptoms of abdominal pain and tenderness, or symptoms and signs of local compression.
This case demonstrates how a rare and potentially life threatening aneurysm manifested as a relatively common presentation – abdominal pain and urinary retention. It is likely that the patient’s urinary symptoms were caused by local compression exerted by the aneurysm and its subsequent rupture.
A triad of symptoms – abdominal pain, urinary retention and haemodynamic instability, prompted the clinician to request urgent imaging thus allowing early intervention and a good outcome. The importance of considering a broad range of differential diagnoses is clearly demonstrated – particularly when more common causes are less likely. This patient had already undergone a TURP making a prostatic cause of retention less probable. Aneurysmal dilation and rupture ought to be among any clinicians differential diagnosis for urinary retention, especially in the context of progressive symptoms in an acutely deteriorating, unstable patient.
There are a number of case reports on the various different presentations of iliac artery aneuryms: lumbrosacral plexopathy, bowel obstruction and a case of a patient presenting with Cullen’s sign. These varied presentations collectively demonstrate the difficultly in swift diagnosis of an internal iliac artery aneurysm with potential associated rupture (5-8). Urological presentations have been infrequently reported in the literature (9,10). The presenting problem in this case report and of those reviewed remains consistent – urinary retention and abdominal discomfort. Haemodynamic instability, as seen in this case, is another indicator that the underlying diagnosis may be vascular in origin. We propose that any patient presenting acutely with urinary retention, abdominal pain and haemodynamic instability should qualify for an urgent CT abdomen in order to rule out an iliac artery aneurysm.
This case emphasises the importance of maintaining a broad and open mind in approach to the management of urinary retention associated with other symptoms, and reacting quickly to clinical developments.

{kind=link}