





Abstract
Pain of the right iliac fossa in young girls can relate to several pathologies of the gastrointestinal and genitor-urinary tract. On the other hand, lymphangiomas in the peritoneal cavity are extremely rare. We report the case of a young woman with pain in the right iliac fossa caused by a cystic lymphangioma. A 17-year-old caucasian female patient presented with abdominal pain in the right iliac fossa and flank of a 1-month duration. The patient was apyrexic and laboratory tests were negative. CT/MRI of abdomen showed a cystic mass (max diameter 60 mm) in the retrocaecl adipose tissue in connection with the caecum and appendix. The patient underwent a total excision of the lesion and appendicectomy. Histopathological examination was consistent with the diagnosis of mesenteric lymphangioma. This case shows a rare but possible cause of right iliac fossa pain in young women to be considered in the differential diagnosis.
INTRODUCTION
Lymphangiomas are rare benign tumors that are preferentially located in the head and neck in children (1). Lymphangiomas in the peritoneal cavity are extremely rare occurring most commonly in the mesentery, followed by the omentum, mesocolon, and retroperitoneum. The etiology is unclear, but they are considered primarily to congenital in origin (2).
We report the case of a young woman with appendicular pain caused by a cystic lymphangioma of the right iliac fossa: a rare but possible differential diagnosis.
CASE REPORT
A 17-year-old female patient presented with a dull abdominal pain in the right iliac fossa and flank of a 1-month duration. An abdominal examination revealed hyperactive bowel sounds and tenderness during palpation in the central abdominal quadrant and right iliac fossa in Mc Burney point. The patient was apyrexial and laboratory tests were unremarkable. Neoplastic markers (AFP, CEA, CA 19-9, CA 15-3, CA125, TPS) were negative.
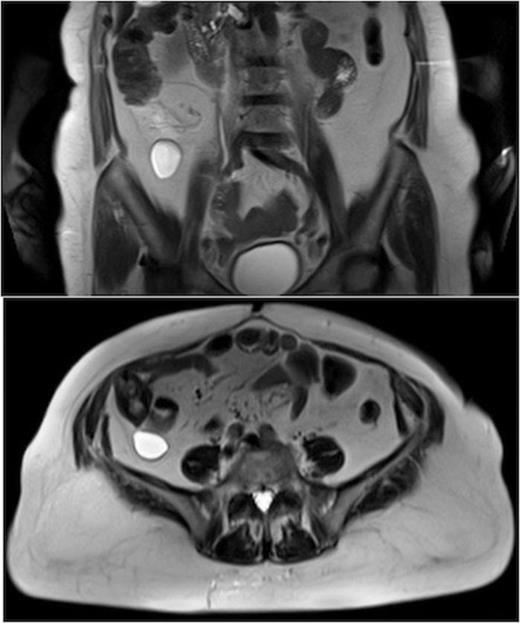
MRI of the abdomen. Axial and coronal T2-weighted TSE images showed the presence of a fluid-filled cystic lesion in the retrocaecl adipose tissue.
An ultrasonographic and CT scan of the abdomen revealed the presence of a cystic mass (max diameter 60 mm) in the retrocaecal adipose tissue that was in proximity of the caecum, appendix and ileum. In addition, the CT scan revealed the presence of multiple hypodense formations in the body and tail of pancreas.
During the hospital stay an abdominal MR was performed. The exam revealed in the retrocaecl adipose tissue the presence of a fluid-filled formation with a diameter of 60 mm that appeared indissociable from the caecum for the presence of a tissue connection (Fig 1). Other cystic lesions (communicating with pancreatic duct) were present in the whole pancreas and in the right kidney.

Fluid-filled cystic lymphangioma with polycyclic edge and internal septa (intraoperative specimen)
The patient underwent exploratory surgery: at laparotomy a yellowish oval formation with a diameter of 6 cm was found arising from the mesentery of terminal ileum with partial adhesion of the appendix. The lesion had a cystic aspect and was fluid-filled (Fig 2). We performed a total excision of the lesion and appendicectomy. No ileal resection was required. Histopathological examination was consistent with the diagnosis of mesenteric lymphangioma (Fig. 3). The patient has been followed-up for two years with semestral clinical examination and abdominal eco scan and no recurrence occurred.
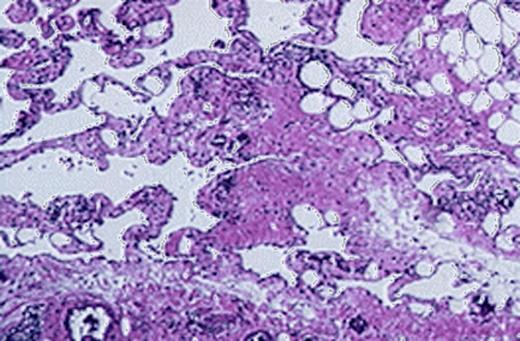
Numerous dilated lymphatic spaces, sometimes filled with lymph and covered by endothelial cells
DISCUSSION
Intra-abdominal mesenteric lymphangioma is an uncommon tumor that usually manifestes in early adulthood. This tumor has an incidence of approximately 1/20,000 and 1/250,000 hospital admissions, and it is more frequent in men than women with a M/F ratio of 3:1 (3). In intraperitoneal sites, the small bowel mesentery (70%) is the commonest localization, with 50–60% of all cysts located in the ileal mesentery. (4)
The etiology of mesenteric lymphangioma is considered to be congenital, with abnormal embryonic development of the lymphatic system causing sequestration of lymphatic tissue (1): infact in our patient also other cystic lesions (kidney and pancreas) were found at abdomen CT/MRI.
Preoperative diagnosis is often difficult due to the frequent silent clinical course. Radiological investigations are a useful diagnostic tool, but definitive diagnosis is confirmed by histopathology after a complete surgical resection. (5) At immunochemistry : the lining mesothelial cells are immunoreactive for cytokeratin and negative for factor VIIIIs. Double staining with Prox1 and CD31 is the most reliable method for characterizing lymphangioma endothelial cells.(6)

{kind=link}
{kind=link}
{kind=link}