





Abstract
Chordoma is a rare, malignant neoplasm thought to develop from the notochord. It most commonly occurs in the base of the cranium or the sacro-coccygeal region but around 15-20% affect the vertebral body. Extra-lesional resection with or without adjuvant radiotherapy is generally accepted as the mainstay of treatment for this slow-growing tumour. We present a case whereby a patient with a solitary L3 vertebral body lesion causing caudal compression was treated with spinal decompression and posterior stabilisation. Pre-operative biopsy was not performed as the lesion was presumed to be a metastatic deposit from a co-existing renal mass. Intra-operative biopsy, however, identified the tumour to be chordoma of the L3 vertebral body which would have been more appropriately treated with ‘en-bloc’ excision. This case highlights the importance of pre-operative tissue diagnosis, and that, although rare (0.8 per 100,000), chordoma should always be considered.
INTRODUCTION
We present a case of chordoma, causing caudal compression, which was initially presumed to be a metastatic deposit from a renal cell carcinoma on the basis of radiological investigations. Consequently the patient received initial surgical intervention in the form of spinal decompression with posterior stabilisation, where extra-lesional resection would have been more appropriate.
CASE REPORT
A 72-year old man presented with an 8-month history of lower back pain and increasing left leg pain and weakness. An abnormal appearance of the L3 vertebral body on plain radiographs prompted CT investigation which suggested pathological fracture of L3 with posterior convexing of the vertebral body and epidural mass. Also noted was a mass within the right kidney which was felt to be in keeping with the appearances of renal cell carcinoma. MRI confirmed a solitary vertebral lesion causing posterior convexity of the vertebral body with extension into the pedicle, causing significant compression of the thecal sac and clumping of nerve roots. The patient was commenced on Dexamethasone. Based on the radiological presumption that this was a secondary deposit from a renal cell carcinoma within the right kidney, plans were made for posterior spinal decompression and stabilisation, and tissue biopsy was felt to be unnecessary. Pre-operative embolization of the tumour was attempted, however, no tumour enhancement was demonstrated during the aortogram, and embolization was therefore not performed. Decompression and posterior stabilisation from T12 to L5 was performed and biopsies of L3 sent for analysis. The biopsy revealed trabecular bone and marrow fat replaced by malignant tumour, in-keeping with chordoma, not the presumed diagnosis of renal cell carcinoma.
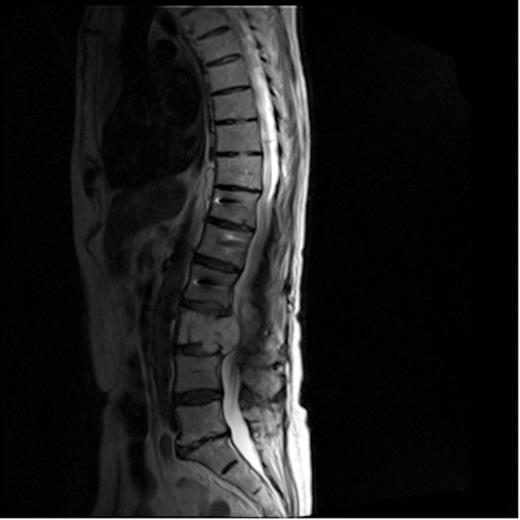
MRI of lumbar spine showing mass causing compression of the cauda
The patient developed an ileus post-operatively but soon settled and his lower back pain gradually improved. Following discharge, a plan was made for further investigation of the renal lesion. Unfortunately his lower back pain returned 6 months later, and subsequent imaging showed enlargement of the lumbar spine mass causing further compression of the cauda. (Figure 1). This subsequently required further surgery in the form of tumour debulking with anterior stabilisation of L3. Investigation of his renal mass is on-going.
DISCUSSION
Thought to arise from cellular remnants of the notochord (the mesodermal precursor of the vertebral column), chordoma is a rare, slow-growing, locally-invasive malignant tumour. The vast majority affect the base of the cranium and sacro-coccygeal region with round 15-20% involving the vertebral body(1,2). It is generally accepted that ‘en-bloc’ surgical excision with wide, tumour-free margins is the treatment of choice. Adjuvant radiotherapy may also be used post-operatively, however Chordomas are relatively radio-resistant and the value of radiotherapy in their treatment is still a matter of debate. Chordomas are well known for their high local recurrence rates following surgery and distant metastases following treatment is reported in greater than 40% of patients (3,4,5,6).
It is extremely rare for chordoma to present in a lumbar vertebral body and this case report highlights an unusual presentation of spinal pathology. Much more common is the presentation of metastatic deposits from a primary tumour elsewhere. In 2005, Patchell et al (7) published their randomised trial which established the superiority of direct decompressive surgery plus post-operative radiotherapy over radiotherapy alone for patients with spinal cord compression from metastatic disease. Since then we have noticed a dramatic increase in the volume of referrals of patients with this condition. In the case of our patient, it was assumed that this L3 lesion was metastatic deposit from renal cell carcinoma based on radiological appearances. Pre-operative biopsy would have established the true nature of the disease process and altered management significantly.
Pre-operative work-up including tissue biopsy and MDT discussion is vital to guide management. Although rare, chordoma and other primary bone tumours should always be considered as a potential diagnosis of a vertebral lesion, despite its location. With our experience of the increasing presentation of spinal metastatic disease, it is important to be aware that primary tumours of the spine still do occur even when pointers to metastatic disease are present. Three dimensional imaging can occasionally be misleading, and diagnostic assumptions cannot always be reliably made based on radiological investigations alone.

{kind=link}