





Abstract
Anomalies of the appendix are uncommon and are usually discovered incidentally during surgery for appendicitis. We present a rare case of appendiceal duplication, which can have serious consequences if overlooked during an operation. Following an initial admission for right iliac fossa pain which led to an uneventful laparoscopic appendicectomy, a 36 year old male was readmitted for increasing abdominal pain and distension. Subsequent surgical exploration revealed a second appendix, which was retrocaecal and gangrenous. Careful inspection of the caecal pole should always be performed during surgery to exclude appendiceal abnormalities such as appendiceal duplication. The Cave-Wallbridge classification exists to provide surgeons with a framework to classify appendiceal duplications.
INTRODUCTION
Although a rare condition, the complications that arise from an overlooked duplicate appendix can have serious, life-threatening consequences for the patient. We present the case of a male patient with a recent history of an appendicectomy, who presented to the emergency department with a gangrenous second appendix.
CASE REPORT
A 36-year old male presented with a 1 day history of right iliac fossa pain. Clinical examination and raised inflammatory makers supported a diagnosis of acute appendicitis and the patient underwent an uncomplicated laparoscopic appendicectomy, though it was noted that the appendix appeared macroscopically normal at the time of the procedure. No other abnormalities were seen. He was discharged 4 days post-operatively. The patient re-presented 7 days later with a three day history of lower abdominal pain, vomiting and abdominal distension. On examination, the patient was febrile, tachycardic and appeared unwell. Inflammatory markers were again elevated. A computed tomography scan revealed a small collection containing gas and fluid just inferior to the third part of the duodenum with a thin tubular structure extending from this collection and ending in the terminal ileum. This raised the possibility of a Meckel's diverticulitis with a localised perforation at the tip. The patient underwent a second laparoscopy, which proved inconclusive and a laparotomy was performed. This revealed a retro-caecal abscess surrounding a second (necrotic and friable) appendix arising from the base of the caecum, which was excised. The appendix stump from the first appendicectomy appeared unremarkable with an intact vicryl suture tied at the base of the stump. The patient's post-operative stay was prolonged due to ileus and pain, and he was discharged 10 days later. Histological examination showed a gangrenous appendix and review of the first resected specimen confirmed a histologically normal appendix.
DISCUSSION
Although variation in the size and position of the appendix is common, duplication is rare and may be associated with other congenital abnormalities (1). Examination of 50,000 histological appendix specimens revealed just two instances of congenital duplication (2). The true incidence of duplicated appendix is estimated at 0.004% (1,3). This condition must be distinguished from a solitary diverticulum of the caecum, which is found on the inner aspect of the ileocaecal angle and does not contain lymphoid tissue histologically (4).
The Cave-Wallbridge classification (4) exists based on reported cases and divides appendix duplications into three types (figure 1):
Type A: Single caecum with one normally localised appendix exhibiting partial duplication
Type B: Single caecum with two completely separate appendices and divided into two further subgroups. Type B1 (“bird-like type”): two appendices located symmetrically on either side of the ileocaecal valve, resembling the normal arrangement in birds. Type B2 (“taenia-coli” type): one appendix arises from the caecum at the usual site and the second branches at varying distances along the lines of the taenia from the first.
Type C: Double caecum, each bearing its own appendix.
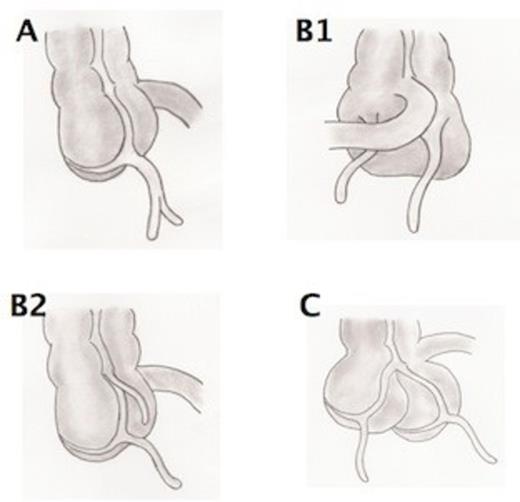
Cave-Wallbridge Classification: Type A: Single caecum with one normally localised appendix exhibiting partial duplication. Type B1: Two appendices located symmetrically on either side of the ileocaecal valve. Type B2: One appendix arises from the caecum at the usual site and the second branches at varying distances along the taenia from the first. Type C: Double caecum, each bearing its own appendix.
Our case was type B2, the most frequently encountered duplication. Although rare, the potential complications of missing a duplicate appendix may have serious, life-threatening complications for the patient. In the case described, the patient experienced significant morbidity in terms of readmission to hospital, further surgical procedures and prolonged hospital stay. Surgeons performing appendicectomies should be aware of the possibility of a duplicate appendix, particularly in the context of an unwell patient with clinical features highly suggestive of acute appendicitis, but with a macroscopically normal appendix at the time of operation. Consequently, the caecum should always be inspected carefully to exclude appendiceal abnormalities.

{kind=link}