





Abstract
Bowel perforation can be potentially fatal. We describe the case of a 42-year-old male who presented with severe abdominal pain following anal fisting. Clinical examination revealed tenderness of the complete abdomen with signs of peritonism. A CT-scan with rectal contrast showed a perforation of the sigmoid 40 cm above the anus. At laparoscopy, a perforation in the sigmoid colon was found and successfully repaired. Patient recovered uneventful and was discharged in 5 days. We present a unique case of a sigmoid perforation after anal fisting which was laparoscopically repaired without formation of a protective colostomy.
INTRODUCTION
In men having sex with men high risk sexual behavior can be seen. Often with concomitant use of recreational drugs such as ecstasy, cocaine, ketamine, and poppers. (1,2) Activities include fisting and unprotected anal intercourse. Also transanal introduction of foreign bodies is a well known phenomenon.
Bowel perforation as a complication of such activities can be potentially fatal. The treatment of a bowel perforation is most commonly performed by laparotomy. (3) Procedures which can be performed in such patients are suturing of the perforation with or without formation of a protective colostomy, a Hartmann procedure or bowel resection with primary anastomosis. (3)
Bowel perforation can also be caused as a complication of a colonoscopy. The risk of perforation after colonoscopy is small, around 0.12%. (4) The retrieval of upper gastro-intestinal foreign bodies and bowel perforation after colonoscopy can be managed by laparotomy or laparoscopy (5,6), although complex complications due to foreign bodies in the rectosigmoid are usually managed by laparotomy. (1) Here we present a case of a laparoscopic repair of a sigmoid perforation due to a foreign body, in this case a human fist after anal fisting.
CASE REPORT
A 42-year-old HIV-infected man presented himself to our emergency department with severe abdominal pain five hours following anal fisting. Clinical examination showed an agitated male with no tachycardia, hypotension or fever. Physical examination of his abdomen revealed tenderness of the complete abdomen with signs of peritonism. A plain abdominal radiograph was reported to have normal findings. Laboratory results showed no abnormalities. Based on his clinical condition, a CT-scan with rectal contrast of the abdomen was performed. The CT-scan showed a perforation of the sigmoid 40 cm above the anus.Figure 1 shows rectal contrast throughout the complete abdomen as high as the diaphragm.
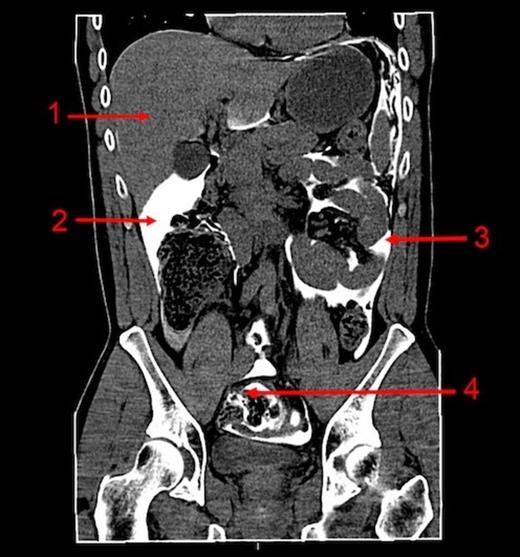
CT abdomen (coronal) with rectal contrast:1. Liver, 2. Contrast in the sub hepatic region, 3. Contrast in the left abdomen, 4. Sigmoid with extra luminal contrast
Under general anesthesia patient underwent a laparoscopy in which a defect of the sigmoid was found with only minimal signs of local peritonitis. The defect had a diameter of 9 centimeters and was located approximately 20 cm above the transverse rectal fold (figure 2). Because of the absence of general fecal peritonitis we opted to suture the perforation in two layers with a Vicryl 2.0, without formation of a protective ileostomy. Patient made an uneventful recovery and was discharged in 5 days.
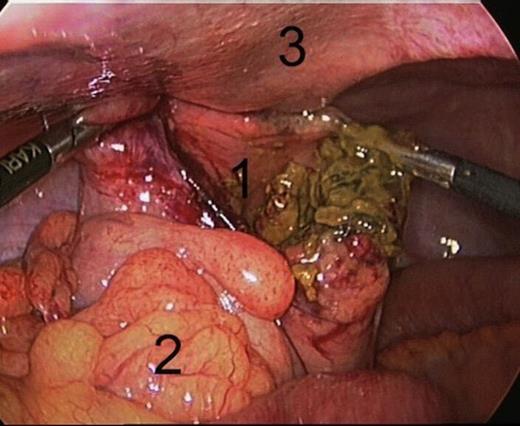
Laparoscopy: defect of the sigmoid:1. Large defect of the Sigmoid, 2. Sigmoid mesocolon, 3. Abdominal wall
Patient was frequently reviewed in our outpatient department. At the time of the last telephone contact with the patient he had made a complete recovery without any sequelae of his abdominal surgery.
DISCUSSION
A large bowel perforation can be potential fatal due to the development of peritonitis by contamination of the peritoneal cavity. This can lead to a septic shock, which requires immediate surgery. There is a high risk of mortality and morbidity in patients with a septic shock due to peritonitis caused by bowel perforation. (7) Most common causes of colon perforation which lead to peritonitis are colorectal cancer and complications of colonic diverticulitis representing between 64% and 100% of cases with peritonitis due to different etiologies. (8) In literature the incidence of iatrogenic colon perforation after colonoscopy, which also can lead to peritonitis, has been described between 0.06 % and 0.1 %. (9)
Laparotomy was always considered to be the first choice to manage colon perforation due to its advantages such as adequate localization of the perforation, closure or repair of the defect and the possibility for peritoneal lavage. A more recent study showed that outcomes in laparoscopic repair of colonic perforation are the same as in open surgery. (5)
In our patient, we performed a successful laparoscopic repair of his sigmoid perforation. Because of the short time (7 hours) between the trauma and surgery we decided to only suture the large defect without a protective ileostomy. Laparoscopy has certain advantages compared to open surgery in post-operative outcomes. Less paralytic ileus, faster return to normal bowel function, less pain, lavage of the peritoneum and a shorter duration of hospital stay. (10)
We present a unique case of a sigmoid perforation after anal fisting, which was laparoscopically repaired without formation of a protective colostomy. Laparoscopic repair of traumatic colon perforation, for example after colonoscopy, can be performed in experienced surgeons.

{kind=link}
{kind=link}