





Abstract
Trans-mesenteric hernia is a form of internal hernia which is an extremely rare cause of intestinal obstruction in adults compared with the pediatric population. It often presents with complications such as acute intestinal obstruction and peritonitis requiring immediate surgical intervention. We report a case of a 21-year-old woman who presented to us with an acute abdomen and peritonitis that required an immediate exploratory laparotomy. She was found to have a small congenital mesenteric defect with strangulated segment of ileum. Gangrenous portion of the ileum was resected and the congenital defect was closed. The patient made an uneventful recovery. The occurrence of trans-mesenteric hernia in adults is rare and difficult to be diagnosed clinically; thus, the patient's clinical features may lead to early surgical intervention in order to reduce morbidity and mortality.
INTRODUCTION
An internal hernia is defined as the protrusion of a viscus through a normal or an abnormal opening within the boundaries of the peritoneal cavity.
Trans-mesenteric hernia is a type of internal hernia which is an unusual cause of bowel obstruction. It may result in irreversible damage of the bowel and a fatal outcome. Less than 1% of the cause of small bowel obstruction is due to internal hernia [1, 2].
Paraduodenal hernia continues to be the most common type of internal hernia (50%) in the abdomen without prior surgery [3, 4] compared with trans-mesenteric hernia in which the incidence ranged from 8 to 10% [5, 6].
Most of the reports of congenital trans-mesenteric hernia involve the pediatric population but even in this group of patients, the trans-mesenteric defect is infrequent [7, 8].
CASE REPORT
A 21-year-old woman who was otherwise healthy before presented with severe abdominal pain. The pain was generalized, severe, acute onset and continuous. She was also found to have multiple episodes of vomiting for a period of 24 h. Otherwise, she had no fever, no history of previous abdominal surgery, no other co-morbids and no trauma.
On examination she was drowsy, tachycardic with a pulse rate of 120 beats/min, BP 130/78 mmHg, temperature 37.0°C, dehydrated and respiratory rate of 24 breaths/min. An abdominal examination revealed distended abdomen, generalized abdominal tenderness and guarding. Bowel sounds were absent.
Laboratory investigations results were normal, except for an elevated white blood cell count of 16 000/mm3.
In view of generalized peritonitis, the abdomen was explored through an emergency midline laparotomy after initial resuscitation.
Upon entering the peritoneal cavity, 2 l of hemorrhagic fluid was drained. A loop of ileum had herniated through a small mesenteric defect. A total of 180 cm ileum noted to be gangrenous with loss of peristalsis and absent pulsations (Fig. 1). Terminal ileum and the ileocecal junction were also nonviable. Pulsations of mesenteric vessels were intact. The mesenteric defect measuring 3 × 3 cm located about 4 cm from the mesenteric edge of mid-jejunum. There was no evidence of malrotation. A limited right hemicolectomy with extensive gangrenous small bowel resection was performed and a stapled side-to-side functional anastomosis created. The mesenteric defect mentioned earlier was closed with interrupted sutures. The patient recovered well from the surgery. She was allowed orally on day 3 post surgery (Figs 2–4).

Gangrenous ileum found on emergency exploratory laparotomy.

Ileum herniated through congenital mesenteric defect.
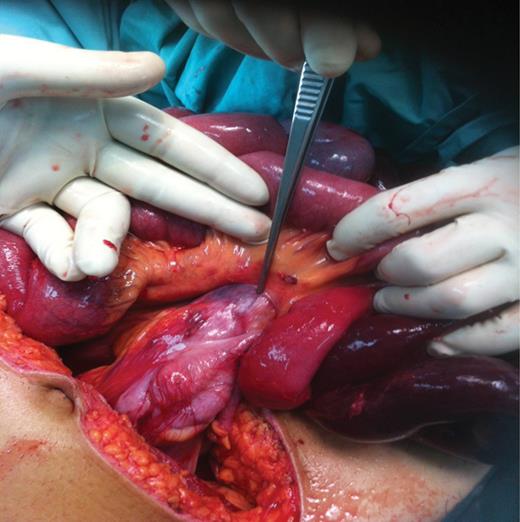
Herniation caused gangrenous terminal ileum.

Congenital mesenteric defect at mid-jejunum.
DISCUSSION
Congenital defects in the mesentery have been described as an uncommon pathology, presented mainly in the pediatric population [9] and these are very rare in adults.
However, in this case we are reporting the mesenteric defect to be congenital and the cause for the bowel strangulation. Defects are most commonly acquired in adults as a result of either blunt abdominal trauma or surgical manipulation of the bowel and mesentery.
Most of the literature reports that the most common form of presentation is an acute intestinal obstruction which is also the clinical presentation of our patient. It could be an intermittent obstruction as well, which delays the diagnosis and treatment [8, 10].
As it is an uncommon etiology for intestinal obstruction most of the congenital mesenteric hernia diagnoses are made during the operative time.
Most of the time clinical features such as peritonitis and acute intestinal obstruction warrant for an immediate surgical intervention.
Morbidity and mortality of the condition depend mainly on the time of onset, clinical severity, the patient's co-morbidities and vascular compromise.
Conflict of interest statement
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}