





Abstract
Diaphragmatic hernias are usually congenital, and they usually occur in the neonatal group. They do occur in the adult population, albeit very rarely. We present a case of an adult male patient with complications as a result of a congenital diaphragmatic hernia. The patient presented with atypical abdominal pain and respiratory distress. Radiological investigations confirmed a left hydropneumothorax as well as large bowel obstruction secondary to herniation of the omentum and transverse colon through a congenital defect in the left hemi-diaphragm. He had a laparotomy, which confirmed the radiological findings and a perforated transverse colon. He went onto have an extended right hemicolectomy and end-ileostomy; his left hemithorax was lavaged and a thoracostomy tube was inserted. He recovered well, except that he developed an empyema postoperatively for which he required a thoracotomy and decortication. He made good recovery following this and was discharged home nine days following his initial laparotomy.
INTRODUCTION
Diaphragmatic hernias are commonly congenital, and they predominantly involve the very young neonatal group. However, there are adults who present with symptomatic diaphragmatic hernias although their occurrences are rare. A recent article by Kinoshita F et al in fact has demonstrated that the prevalence of these hernias can be as high as 20% among adults, although most of them are asymptomatic (1). For the patients who do present to health care, they are often faced with a delay in diagnosis. Clinical awareness of this uncommon condition should be raised especially when evaluating a patient with respiratory symptoms and atypical abdominal pain, as a delay in appropriate diagnosis and management could result in significant morbidity and mortality.
CASE REPORT
A 39-year-old Caucasian male, with a background history of alcohol excess, presented to casualty with lower abdominal pain, nausea and vomiting. Clinical examination and chest X-ray were unremarkable. Routine blood tests showed mild transaminase elevation. The clinical impression was alcoholic gastritis and he was discharged home.
He re-presented with similar symptoms on three further occasions over the next week. On two occasions he self-discharged after receiving opiate analgesia. On the fourth presentation, he was tachypnoeic (respiratory rate >40/min) and tachycardic (heart rate 130/min). There was reduced air entry over his left hemithorax. His abdomen was distended and tender. His chest X-ray showed a tension pneumothorax on the left with mediastinal shift.
A tube thoracostomy was performed, which drained approximately 300ml of purulent fluid. The follow-up chest X-ray (Fig. 1) showed a persistent pneumothorax although the appearances had improved and the mediastinum was centrally positioned. In view of his on-going abdominal complaints, an abdominal X-ray was obtained. This showed markedly dilated large bowel within the upper abdomen, consistent with large bowel obstruction. A surgical review confirmed him to be distended, tympanic, with upper abdominal tenderness and scanty bowel sounds. A CT scan of the chest and abdomen was requested.

CXR post-thoracostomy
The CT scan showed a left-sided hydropneumothorax with herniation of the omentum and transverse colon through a defect in the postero-lateral left hemi-diaphragm with dilatation of the proximal colon (Fig. 2). Laparotomy confirmed an obstructed diaphragmatic hernia with perforation of the transverse colon into the left hemithorax cavity. The caecum was grossly distended with gangrenous patches and an extended right hemicolectomy with end-ileostomy was performed. Splenectomy was also required for a capsular tear. The left hemithorax was lavaged copiously and a thoracostomy tube placed.
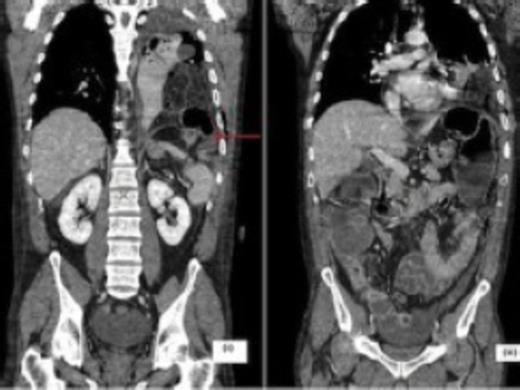
CT scan coronal images depicting the diaphragmatic defect (arrow) with herniation of mesentery and bowel into the left hemithorax (i) and large bowel dilatation proximal to the defect (ii)
Post-operatively, the patient remained pyrexial with a raised white-cell count. Subsequent CT scan confirmed an empyema. He was transferred to the regional cardio-thoracic unit where he underwent a thoracotomy and decortication. He made good recovery following this and was discharged 9 days later.
DISCUSSION
Diaphragmatic hernia occurs as a result of defective closure of the pleuro-peritoneal canal. It is mainly diagnosed in newborns (2), although there are increasingly more adult cases diagnosed incidentally on radiological studies (3). It is more common on the left side as the right pleuroperitoneal canal closes earlier than the left (4). Recent reports have suggested that right-sided hernias are more common than initially thought although they are more often asymptomatic due to the buttressing effect of the liver (3,4). Adult patients are usually asymptomatic. Some may present with vague, non-specific chest or abdominal complaints or as an emergency with strangulation, colonic necrosis/perforation, or a tension pneumothorax (2,4). Concise, detailed history-taking and clinical examination, coupled with raised clinical suspicion, are paramount to prevent missed clinical pathology. When suspected and diagnosed incidentally, referral for consideration of repair should be made as morbidity and mortality following emergency repair is higher than in elective cases (3).

{kind=link}
{kind=link}