





Abstract
The authors report the first known case of Foix-Chavany-Marie Syndrome in a patient with hydrocephalus that reversed with ventriculoperitoneal shunting. A 34-year-old x-ray technician with a history of pilocytic astrocytoma resection and radiotherapy and ventriculoperitoneal shunt placement as a child presented with altered mental status and nausea. She was found to have acute hydrocephalus. Post-operatively she did well and was discharged home. The next day she became acutely altered with anarthria, difficulty speaking, and stiff facial muscles. After multiple revisions, she slowly recovered to her pre-op baseline over the course of next 2 months. This is the first known case of acute hydrocephalus causing Foix-Chavany-Marie Syndrome. Additionally, we show that this unique syndrome is slowly reversible after treatment of hydrocephalus.
INTRODUCTION
The authors report the first known case Foix-Chavany-Marie Syndrome immediately after development of symptomatic acute hydrocephalus that reversed slowly after ventriculoperitoneal shunting.
CASE REPORT
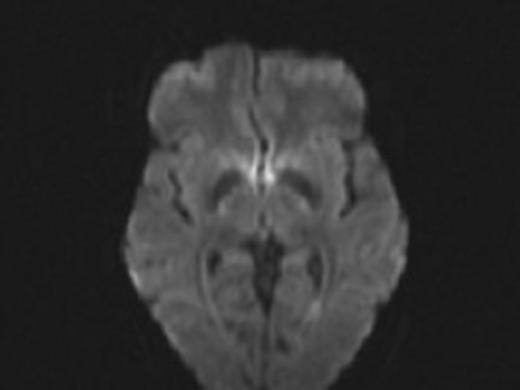
We report the case of a 34-year-old woman with a history of pilocytic astrocytoma resection and radiotherapy with ventriculoperitoneal shunt placement as a child who presented with altered mental status and nausea. She was found to have acute hydrocephalus without any pathology noted on MRI (Fig. 1). She was found to have a shunt fracture at the level of the neck and was taken to the operating room for shunt revision (Fig. 2). At this time, she had an entirely new shunt placed including a programmable valve with an anti siphon device. Post-operatively she did well and was discharged home.

Difussion MRI of the brain prior to syndrome showing no areas of stroke.
Shunt series showing fracture of shunt catheter at neck.
The next day she became acutely altered with anarthria, difficulty speaking, and stiff facial muscles. Involuntary movements such as smiling and blinking of the eyes were preserved. In terms of speech, the best she could do at that time was to produce a high whining sound “uh-uh” or “un-hunh”, without accompanying movement of lips, tongue, teeth, cheeks. She followed commands with her extremities but not with her orobuccal area. On motor exam, she had intact anti-gravity strength in all limbs. She had 3+ reflexes in biceps and patellar tendons, 2+ in ankles and BRs. She had prominent grasp reflexes in both hands, + glabellar reflex, and + palmomental reflex bilaterally. She had negative snout, suck, rooting, and jaw jerk reflexes. She has no impairment in finger to nose other than slow movement. Her cranial nerves were notable for impaired upgaze, but otherwise intact EOMs with slow tracking but no abnormal saccades and no nystagmus. There was intact facial sensation bilaterally. There was no voluntary movement of her cheeks, lips, tongue, or oropharynx. Her jaw muscles were quite stiff.
She was diagnosed with Foix-Chavany-Marie Syndrome. Scans demonstrated acute communicating hydrocephalus (Fig. 3). She was taken back to the operating room 7 days later after further workup was negative for a shunt revision to a medium pressure valve without an anti siphon device. She remained neurologically the same. Her scans showed continued ventricular enlargement and she required another trip back to the operating room for a new ventricular catheter.

CT scan showing acute enlargement of the ventricles post initial revision demonstrating shunt failure
Thereafter, her ventricles diminished in size back to their baselines and her neurological exam slowly improved back to her baseline over the course of 2 months. She had no lesions noted in the opercular regions on her MRI post operatively (Fig. 4).
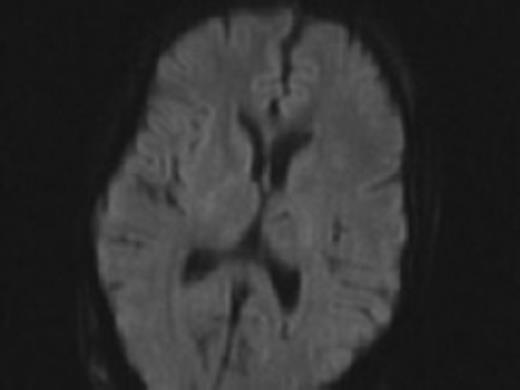
Diffusion MRI showing no strokes post operatively
DISCUSSION
Foix-Chavany-Marie syndrome was first described in 1837 by Magnus and later instituted in 1926 by Foix et. al (1). It is also known as opercular syndrome or facio-labio-pharyngo-glosso-laryngo-brachial paralysis (1-4). This unique syndrome is characterized by continued reflexive movements of the face with loss of voluntary movements of the facial, lingual, and pharyngeal muscles. Thus emotional and reflexive movements in these muscles, as well as limb strength, are preserved. Writing and comprehension is preserved as well (5).
The cause of this syndrome has been well documented to be associated with bilateral opercular and peri-sylvian injury (6). The causes reported stem from vascular injury such as stroke, trauma, and infection (6). Weller et. al. described five categories of this syndrome: a) Classical form due to cerebrovascular disease, b) infectious cause, c) neuronal migrational disorders, d) epilepsy induced, e) neurodegenerative disorder related (5). There is a report of progressive dysarthrophonia of the bulbar type with mild word-finding difficulty that was inititally misdiagnosed to be of psychogenic origin but later interpreted as this syndrome (7). Duffau et al reported a case of this syndrome post resection of a right insulo-opercular low grade glioma (8).
This is the first known case of this syndrome caused by hydrocephalus and relieved with ventriculoperitoneal shunting. We feel that the stretch of the frontotemporal opercular fibers from acute hydrocephalus caused this syndrome and perhaps tolerance for this was lessened by previous radiation treatment in her youth. Perhaps further studies with diffusion tensor imaging may elucidate this hypothesis. Over the course of the next two months, our patient slowly improved. This syndrome should be considered on the differential diagnosis list in patients with the above symptoms who have had acute hydrocephalus. Additionally, this syndrome likely caused by hydrocephalic stretch of bilateral opercular fibers shows gradual recovery, as seen in our patient over the 2 month period.

{kind=link}
{kind=link}
{kind=link}
{kind=link}