





Abstract
Strumal carcinoid develops in a germ cell tumor characterized by an intimate mixture of thyroid and carcinoid. Unlike other carcinoid tumors, most patients with strumal carcinoid have no symptoms of carcinoid syndrome; few are reported to cause severe constipation.
We report a case of a 60-year-old female patient presenting with severe progressive constipation and painful defecation for last few years. A right ovarian tumor was discovered during clinical examination. CT scan revealed a large lobulated solid cystic right adenexal mass suggestive of monomorphic teratoma, which was successfully removed surgically. The histopathology confirmed the diagnosis of strumal carcinoid tumor. Her constipation completely disappeared post surgery. These tumors are known to produce a biologically active substance like peptide YY, which has a pharmacologic inhibitory action on intestinal motility. This was presumably the cause of the constipation in this patient rather than a mechanical effect of the tumor.
INTRODUCTION
Primary ovarian carcinoids comprise 0.1% of all ovarian malignancies and approximately 0.5–1.7% of all carcinoid tumors (1, 2). Strumal carcinoid is a type of germ cell tumor characterised by an intimate mixture of thyroid tissue and carcinoid with other teratomatous elements present in 80% of cases.(3) Most patients with strumal carcinoid have no symptoms of carcinoid syndrome like flushing and diarrhoea, but on the contrary few are reported to cause severe constipation (4). We report a rare case of a postmenopausal lady presenting with severe progressive constipation probably due to monomorphic ovarian teratoma, suspected preoperatively due to presence of severe constipation not attributed to any other cause. After surgery the intractable constipation improved dramatically.
CASE REPORT
A 60 yrs old postmenopausal lady was referred to our outpatient department with a complex right adnexal mass for surgery.
She had chronic constipation for the last 3 years and pain at defecation for the last 9 months. Constipation increased over the last year with stool passage once every 4 to 5 days. She was not suffering from any chronic medical or surgical illness. Her abdomen was soft and distended while bimanual examination revealed a normal uterus and a 5×6 cm cystic firm mass felt through right fornix with limited mobility. Ultrasound showed a solid right adnexal tumor with mixed echogenicity and increased blood flow. Routine investigations including serum electrolytes and thyroid function test were all within normal limits. Serum tumor markers such as CA125, carcinoembryonic antigen and lactate dehydrogenase were within normal limits. Stool occult blood test for three consecutive days was negative.
Computed tomography showed a large lobulated solid cystic 5×9 cm mass in right adnexa which was well defined, bosselated and had hyper vascular enhancement with fatty component and calcific foci suggestive of a teratomatous mass. Distended large bowel loops and a subcentimeteric retroperitoneal lymph node were noted. Colonoscopy was planned but could not be done due to impacted bowel.
According to the clinical and imaging information and postmenopausal status of the patient possibility of a solid ovarian teratoma was considered and after discussion with the patient and her family exploratory laparotomy was planned.
Laparotomy revealed a 6 x 8 cm tumor arising from the right ovary with bosselated appearance, firm consistency and intact capsule. The tumor was adherent to the lateral pelvic wall by thin adhesions, but did not adhere to or compress the colon. Uterus, left ovary and both tubes were normal. There was no ascites and the colon was distended. Because the malignant potential of the tumor could not be ruled out pan hysterectomy was done.
On gross examination, the tumor was 8 x 6 x 4 cm, yellowish brown in color with bosselations on the surface and vague nodularity. Cut section revealed predominantly solid mass with few cystic areas, with one of the cysts showing a tuft of hair. On histopathologic examination the cystic spaces were lined by skin with underlying adnexal structures (Figure 1a). The solid areas showed a population of monomorphic cells with moderate amount of eosinophilic cytoplasm, arranged in acinar, trabecular and glandular patterns suggestive of a carcinoid (Figure 1b,1c). In addition focally follicular structures with central dense eosinophilic colloid like material were seen (Figure 1d) Based on the presence of these two components a diagnosis of Strumal Carcinoid was made and confirmed on immunohistochemistry. The tumor cells were diffusely immunopositive for synaptophysin (Figure 1d), chromogranin and the follicles including the central colloid were immunopositive for thyroglobulin (Figure 1e).
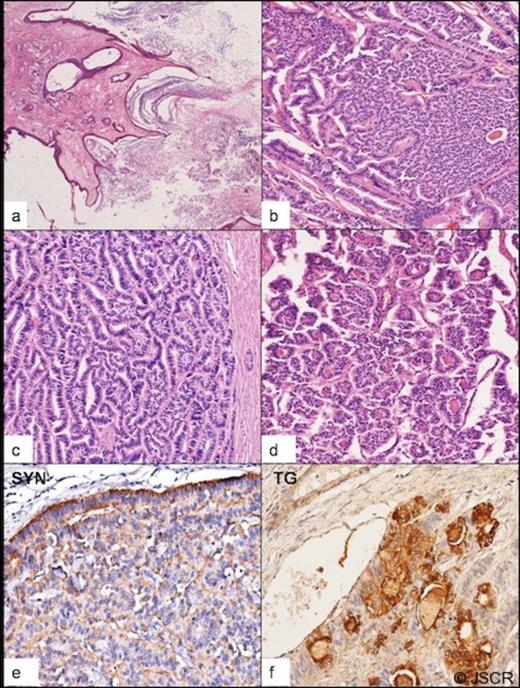
Panel depicting microscopic findings: Ectodermal component in the form of skin and underlying adnexal structures lined the cystic spaces ( a, 4x H&E). Monomorphic tumor cells in a variety of neuroendocrine architectural patterns including acinar and trabecular arrangements were seen ( b, 10x H&E; c, 20x H &E) At places colloid filled follicles were identifiable ( d, 20x H &E). Immunohistochemistry showed diffuse cytoplasmic reactivity for synaptophysin throughout the tumor ( e, 20x) and focal cytoplasmic reactivity for thyroglobulin which also stained the central colloid ( f, 20x)
The patient progressed well in the postoperative period and had her first bowel movement several hours after surgery. The constipation improved dramatically and she passed stools every day. At 6 months follow up, she was having regular bowel movements without using laxatives.
DISCUSSION
Functioning ovarian carcinoids are known to cause typical carcinoid syndrome, facial flushing being the most common symptom in approximately 80% cases and two-third of patients have diarrhea (4). Strumal carcinoids on the contrary are usually asymptomatic and 41% are associated with abdominal discomfort due to tumor size or constipation; no patient had symptom of carcinoid syndrome (5). Severe constipation accompanying primary ovarian carcinoid was first reported by Motoyama et al in 1992, indicating that the constipation may be caused by an inhibitory substance, produced by the tumor and not by the mechanical effect of the tumor mass (6). It is a polypeptide hormone consisting of 36 amino acids and is called peptide YY (PYY) because it is a polypeptide having an N- terminal tyrosine (Y) and a C- terminal tyrosine (Y) (7). It is normally secreted by the neuroendocrine cells in the mucosa of the gastro intestinal tract, especially the colon, ileum and pancreas. It is known to have many biologic effects like inhibition of gastric acid and pancreatic exocrine secretion, gastric emptying and intestinal motility. Excessive peptide YY secreted from a primary ovarian carcinoid may enter the systemic circulation without first pass metabolism in the liver, and may cause severe constipation.
As the constipation improves dramatically after complete tumor resection; a PYY like substance must be the most likely element that interfered with intestinal motility (8)
Shigeta et al showed that a primary ovarian strumal carcinoid is suggested to express complete PYY mRNA and 50%-70% of these cells express PYY antigen (7). Later Kawano et al described strumal ovarian carcinoid in a patient presenting with severe progressive constipation with sudden improvement after resection of tumor. Immunohistologic staining showed the presence of PYY in the carcinoid cells (9).
Our patient, a postmenopausal lady suffered from pain abdomen and severe progressive constipation for 3 years with a solid right ovarian tumor. Clinically we could have measured serum peptide YY but this test is not available in our institute and we did not measure serum 5-HIAA as the patient did not present with symptoms suggestive of carcinoid syndrome.
Overall, the reported survival for patients with disease confined to one ovary is excellent and 65% of these tumors are confined to stage I disease [5]. Complete resection remains the standard management of a primary ovarian carcinoid tumor, and thus far, there is no evidence to support adjuvant chemotherapy or radiotherapy for treatment of carcinoid tumors.
Measuring serum PYY might be a reliable way to monitor tumor status; recurrence is usually manifested as severe constipation. Matsuda et al reported that a 50-year-old woman experienced constipation again 10 months after resection of a stage Ia strumal carcinoid tumor and showed recurrence (10). We believe serum PYY might be used as a tumor marker in the diagnosis and monitoring of this distinctive hormone producing tumors, especially when the symptom is severe constipation rather than diarrhea or flushing.
This case adds to the rare report in the literature of severe constipation probably due to an ovarian strumal carcinoid tumor, which was suspected before surgery. Our patient had dramatic relief of severe constipation soon after surgery, which suggested complete removal of the strumal carcinoid tumor. In any patient presenting with chronic progressive constipation and an ovarian tumor, a strumal ovarian carcinoid should be considered in probable diagnosis.

{kind=link}