





Abstract
Myxomas are the commonest primary cardiac tumours. They may be asymptomatic, and picked up incidentally, or be the cause of congestive heart failure, arrhythmias and/or murmurs. Echocardiography is necessary for diagnosis. Surgical resection is recommended to prevent further complications. A rare symptomatic ventricular myxoma is presented in this case report.
INTRODUCTION
The commonest neoplasms of the heart are metastatic (autopsy frequency 1.5-21%). Primary cardiac tumours have an autopsy frequency of 0.001% – 0.28%. Three-quarters of these are benign and three-quarters of these are myxomas.(1)
Myxomas most commonly occur in the left atrium (90%) and are generally attached to the atrial septum in or adjacent to the fossa ovalis. They can also be found in the right atrium, or right or left ventricles. They tend to present in the age group 30-60 years, and more commonly in females.
Multiple myxomas can occur, but they tend to be familial. Familial myxomas account for 10% of all cardiac myxomas. ‘Syndrome myxoma’, a genetic disorder should be suspected in individuals who are under 40 years of age with multiple myxomas.(1) Carney’s complex, a neuroendocrine-cardiac syndrome is a common cause of familial recurrent cardiac myxomas. Other characteristics include pigmented skin lesions, schwannomas and multiple recurrent mucocutaneous myxomas, and endocrinal neoplasms/overactivity.(2)
Myxomas may be asymptomatic (these being picked up incidentally on routine echocardiography or other imaging). Common symptoms and signs, however, include dyspnoea, palpitations and heart murmurs. Obstruction of a heart chamber by a large myxoma may lead to transient loss of cardiac output with syncope and pulmonary hypertension, resulting in pulmonary oedema and breathlessness. Fragments of the tumour may also embolise causing systemic constitutional symptoms such as fever and arthralgia.(1,3)
Structurally most myxomas have a stalk, and are gelatinous with a broad base. The surface may be either friable or villous.(4) Histologically, they are made up of polygonal multipotential mesenchymal cells which are found in the subendocardium. These cells are thought to be neuroendocrine in origin, and have the ability to differentiate into fibroblasts, smooth muscle cells, endothelial cells and neuroendocrine cells.(2)
Diagnosis of cardiac myxomas is usually made using Transthoracic Echocardiography (TTE), which has a 95.2% detection rate. Alternatively, Transesophageal Echocardiography (TEE or TOE) can also be used.(1)
CASE REPORT
We present a 42 year old female who was referred to the cardiology service by her GP. She reported a 5 week history of New York Heart Association (NYHA) functional classification Class II – III dyspnoea, a generalised lack of energy and a ‘flu-like’ illness, with cough, for which her GP prescribed antibiotics.
She also reported a 3 week history of bilateral leg swelling. 3 weeks prior to presentation, she experienced a TIA-like episode, with right-sided facial and upper limb weakness, and dysarthria. This episode lasted about 30 minutes.
On examination, a soft (2/6) systolic murmur was heard over the right sternal edge. JVP was not raised and no carotid bruits were heard. Neurological examination revealed no abnormalities.
Echocardiography revealed a very large lobulated heterogenous mass in the right ventricular apex. A further mass or extension of this was also seen in the right ventricular outflow tract. This extension was mobile and had a homogenous texture. MRI and CT Thorax (Figures 1 & 2) demonstrated a 4.1cm x 9cm x 4.1cm lobulated mass within the right ventricle, obstructing the right ventricular outflow tract.
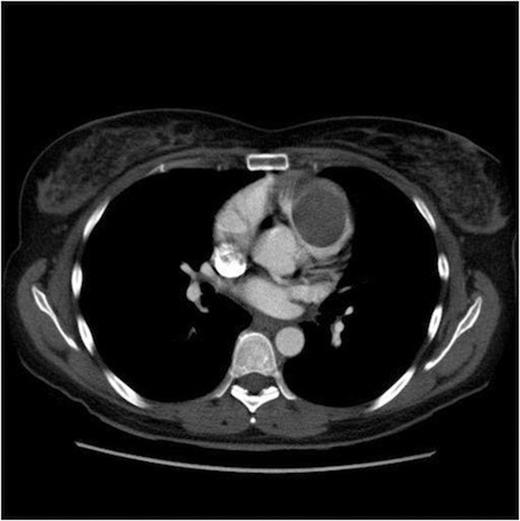
CT Thorax demonstrating a mass within the right ventricle

MRI Thorax demonstrating the same mass as in Figure 1
Patient was referred for urgent surgery. At surgery under cardiopulmonary bypass, the right ventricle was explored through incisions in the right atrium, and in the infundibulum. An 8 cm x 7 cm mass was found to be attached to the inflow of the right ventricle (the anterior tricuspid leaflet) and the apex. It was virtually occluding the outflow of the right ventricle. A further incision in the apex of the right ventricle was required to resect the tumour with all its attachments. The anterior leaflet of the tricuspid valve was excised and the valve reconstituted as a bicuspid valve.
The patient made a full recovery and discharged 5 days after surgery. Histology confirmed complete excision of a myxoma. (Figure 3)

The resected ventricular myxoma
DISCUSSION
Cardiac myxomas are a rare cause of various signs and symptoms and should be considered in the differential diagnosis. Some are picked up incidentally. Whatever the presentation, the management of a myxoma remains prompt surgical resection to prevent embolisation or occlusion of an intracardiac valve. Surgical outcomes are very good, with a 5% risk of recurrence. (1) Recurrence has been noted to be higher in familial myxomas. (2)

{kind=link}
{kind=link}
{kind=link}