





Abstract
Several methods of femoral hernia repair have been described. It is the one most likely to strangulate, its repair must often be accompanied by examination of, and sometimes resection of, bowel or omentum. We describe a new method to repair such a hernia.
INTRODUCTION
Several methods of femoral hernia repair (1,–,5) have been described. It is the one most likely to strangulate (4), its repair must often be accompanied by examination of, and sometimes resection of, bowel or omentum (4). The low skin-crease approach of Lockwood allows easy access to the hernial orifice, but a separate laparotomy incision is required if any of the abdominal contents are to be resected or examined.
Lotheissen (1878) described the high approach through the posterior wall of the inguinal canal; its disadvantage is the increased incidence of subsequent direct inguinal hernia through the disrupted posterior wall. McEvedy’s (6) approach through the rectus sheath (1950) with a vertical para-rectus skin incision avoids this disadvantage and offers good exposure of the femoral canal and abdominal contents. A modification using a skin crease incision instead of a vertical one was proposed by Mouzas/Diggory (2) (1956).
Many patients with femoral hernia in whom strangulation (6,8) is suspected are elderly and infirm. A single incision is to be preferred, especially as it can be performed under local anaesthetic (2) with minimum disruption and disadvantage.
SURGICAL TECHNIQUE
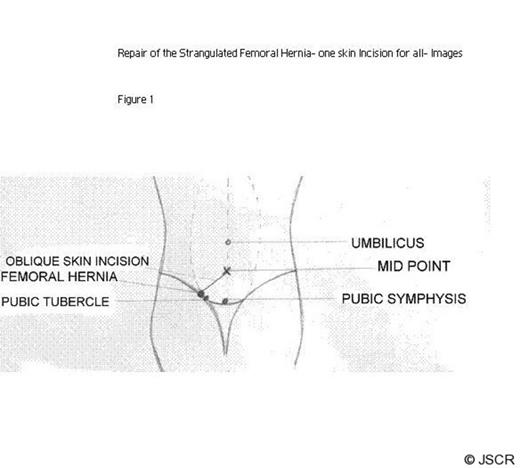
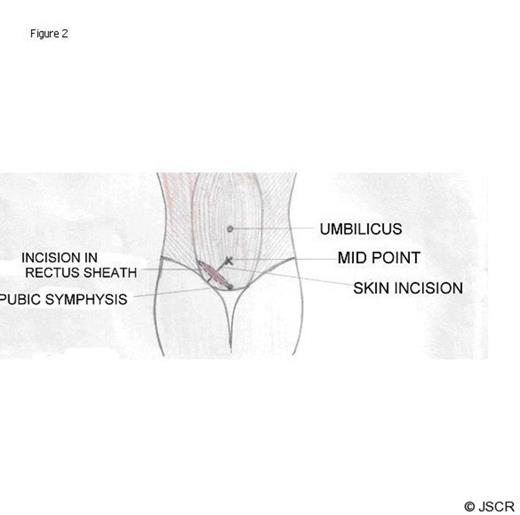
An oblique skin incision of about 6 – 8 cms is made from the hernial bulge itself to a point midway between pubic symphysis and umbilicus (Figure 1). The anterior rectus sheath is incised at right angles to the skin incision from pubic symphysis extending if necessary into the external oblique (Figure 2). The rectus muscle is retracted towards the midline; it is sometimes necessary to divide the inferior epigastric vessels. The tranversalis fascia is incised and the neck of the sac exposed by finger dissection. The lacunar ligament is divided (with care because of the presence of an abnormal obturator artery at its cresenteric margin in 10%).
At this stage the sac is visible below the inguinal ligament. The sac is opened and the potentially infected collection therein is drained before the peritoneal cavity is opened. The hernia is then reduced and the neck of the sac is excised. A general inspection of the peritoneal cavity is carried out and any resection performed, if needed. The peritoneum is closed using an absorbable suture. The femoral canal is repaired from inside by approximating the inguinal ligament to the pectineal ligament with interrupted non-absorbable sutures. Care should be taken to avoid damage to the femoral vein (repair of the right femoral canal is best done standing from the left side of the patient, but repair of the left femoral canal is best done standing from the left side). The rectus sheath is closed with absorbable sutures, and the skin closed with sub-cuticular absorbable sutures. All patients should have a urinary catheter in-situ during the operation and routine DVT prophylaxis. Antibiotics are not given routinely.
Thirty-five femoral hernias with suspected strangulation were repaired by this method. In ten, bowel resection was necessary; local anaesthesia was used in nine of these. In the other twenty-five thorough examination showed the bowel to be viable. All the wounds have healed well apart from two in which infection developed; these responded to antibiotics. All patients were followed up for two years and neither recurrence nor incisional hernia occurred.
DISCUSSION
This approach can be used in all cases in which strangulation (4) is suspected, as both hernia repair and bowel resection can be done through the same incision.
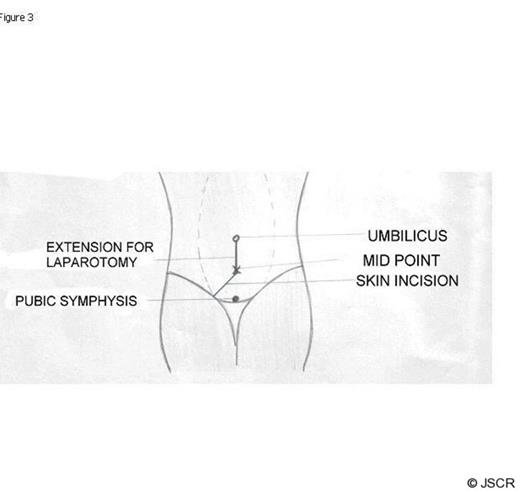
The incision can be converted into a midline laparotomy by extending it proximally in the midline (Figure 3). The femoral canal is better repaired from inside and hence the chance of recurrence is greatly reduced.
The chance of incisional hernia developing is greatly reduced as the skin incision and rectus sheath incision are at right angles reinforcing each other. This operation is suitable for local anaesthesia (2) even if resection of the bowel is needed, an advantage as many patients are elderly, infirm and unfit for general anaesthetic.

{kind=link}
{kind=link}
{kind=link}