





Abstract
Littoral cell angioma (LCA) is a rare benign splenic vascular neoplasm. We report a case of a 58-year-old man with a 5.5-cm lesion in the upper pole of the spleen. A laparoscopic partial splenectomy was performed. He was discharged on the second postoperative day. Pathology revealed LCA.
Laparoscopic partial splenectomy can be performed safely in selected cases and is an appropriate option in patients with benign conditions as it enables preservation of the immunologic function of the spleen. Long-term follow up in patients with LCA is important given its high association with other malignancies.
INTRODUCTION
Total splenectomy is associated with an increased risk of overwhelming infections (1) and arterosclerotic events (2), and spleen-preserving approaches have been employed in selected cases of open elective surgery as well as trauma (3). Laparoscopic partial splenectomy (LPS) has been successfully applied recently in selected patients, particularly children, with splenic cysts, benign tumors, splenic infarcts and in children with splenomegaly (1,4,–,6).
Littoral cell angioma (LCA) of the spleen is a rare benign vascular tumour that arises from the littoral cells in the splenic red pulp sinuses. We present a case of LCA of the spleen treated successfully with LPS.
CASE REPORT
A 58-year-old Caucasian man presented with chest pain, on a background of type-II diabetes mellitus, hypertension and hypercholesterolaemia. A Cardiologist excluded ischaemic heart disease. Full blood count was normal, and an ultrasound scan of the abdomen revealed a 5.5-cm splenic lesion. Computed tomography (CT) revealed a 55mm X 36mm hypodense lesion in the upper pole of the spleen, while magnetic resonance imaging (MRI) demonstrated a well-circumscribed exophytic round mass arising from the anterior aspect of the spleen with features compatible with a benign solid tumour of uncertain malignant potential and multiple liver haemangiomas [Figures 1 and 2]. We proceeded to LPS after the patient had received preoperative vaccinations lest total splenectomy might be necessary.
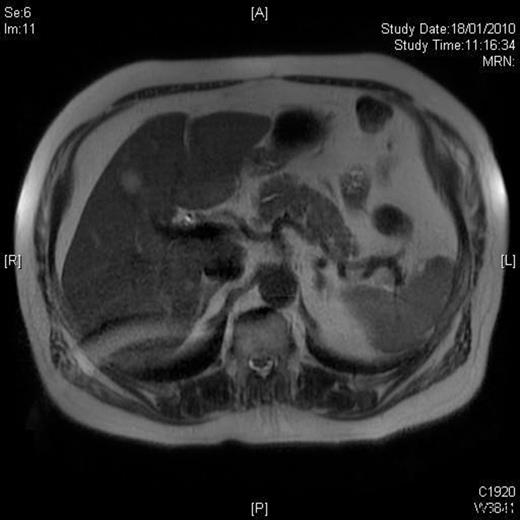
T2W weighted image demonstrating a well circumscribed, round mass arising exophytically from the anterior aspect of the spleen with an intermediate T2W signal intensity.

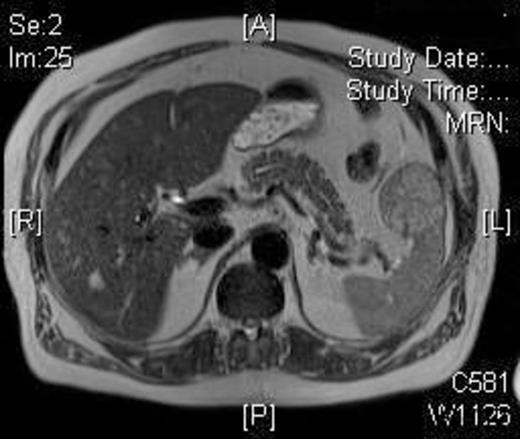
T1W post-gadolinium MRI: the mass demonstrates a degree of late enhancement
The patient was placed in a right lateral position and two 12-mm and two 5-mm ports were applied. A nodule arising from the anterior border of the spleen with a vascular pedicle was identified. The remainder of the spleen was found to be macroscopically normal. The short gastric vessels were divided with an ultrasonically activated scalpel (UAS) (Ethicon Endo-Surgery, Cincinnati, OH, USA). The splenic hilum was dissected and looped with a nylon tape over which a rubber tube was introduced with its outer end protruding through the port wound for approximately 6-cm to facilitate vascular control in case of gross bleeding. The tumour nodule had a distinct vascular pedicle that was divided with the UAS, and this created a line of demarcation between the nodule and the remainder of the spleen that was marked with the UAS. The vascular inflow to the spleen was then clamped by advancing the rubber tube over the Nylon tape and applying a clamp over both tape and tube outside the abdomen. Partial splenectomy was then carried out using the UAS and following the demarcation line. A pro-coagulant (Floseal; Baxter Healthcare SA, Zurich, Switzerland), which consists of a bovine-derived gelatin matrix and a human derived thrombin component, was applied to the cut surface of the spleen. No bleeding from the splenic remnant occurred after the pedicle was unclamped. The specimen was removed intact in a water-impervious retrieval bag after extending one of the 12-mm port wounds.
The operative time was 50 minutes and the blood loss was less than 20 ml. The patient made an uneventful recovery and was discharged on the second postoperative day. Histology demonstrated complete excision of a LCA with no cell atypia. A 3-month postoperative MRI showed no disease recurrence and normal appearance of the splenic remnant [Figure 3].
MRI post-resection: T2W image showing absence of the lesion
DISCUSSION
First described by Falk et al in 1991 (7), LCA appears to affect both men and women equally. Whilst the detection of this tumour in our patient was incidental, LCA may present with hypersplenism and could be associated with malignant tumours in 33% of cases (e.g. adenocarcinoma, renal carcinoma, melanoma, breast cancer, lymphoma, hepatocellular carcinoma, seminoma and papillary thyroid cancer) (8). Some 17% of the reported cases were associated with immunologic or congenital disease such as Crohn’s disease, Wiskott-Aldrich and Evan’s syndrome, virus hepatitis, Gaucher disease and immunosupression by steroids (8).
LCA may appear as multiple or solitary nodule lesion of 1-11 cm (8). The imaging features of LCA are non-specific. Usually the lesion has an echogenic nodular appearance on ultrasound, while a hypodense nodule on CT scan is common to many conditions. A low intensity signal on MRI may be found in only few cases all on sequences due to haemosiderin deposits. In our case, MRI findings have not been diagnostic of LCA and revealed a solid splenic tumour with benign features but an uncertain aetiology and malignant potential. Rarely, the diagnosis has been established preoperatively using percutaneous fine needle aspiration (9). Histologically, these lesions are composed of anastomosing vascular channels with irregular lumina and tall endothelial cells that slough off into the lumina. Cell atypia is absent and mitotic activity is very low, as the case was with our resected lesion.
The treatment of LCA of the spleen is that of laparoscopic or open total splenectomy, particularly when large, of diffuse appearance, or of uncertain nature. To the best to our knowledge, this is the first report of a LPS for LCA. Intraoperative bleeding from the splenic remnant makes LPS challenging, leading to high conversion rate to open surgery (1,4). To achieve vascular control, some authors identified and divided selectively the arterial and venous branches of the splenic pole to be resected (1), while others performed subtotal splenectomy with division of the splenic artery and vein but preserved the upper pole based on the short gastric vessels (5). Others described the use of staples after division of the vascular pedicle to carry out transection of the spleen along the cyanotic demarcation line (4). LPS using radiofrequency ablation has been described by creating a 1-cm thick coagulated parenchyma resection plane that allowed bloodless splenic transection (10). The initial division of the vascular pedicle to the tumour nodule in the technique we describe, the division of the short gastric vessels and clamping of the only remaining vascular inflow to the remainder of the spleen along the splenic hilum, as well as the use of the UAS to transect the spleen along the demarcation line and the application of a pro-coagulant to the cut surface of the spleen resulted in a bloodless procedure.

{kind=link}
{kind=link}
{kind=link}